Cory:
Unlock Your AI Assistant Now!
Ionising radiation is essential in interventional cardiology, but it is associated with occupational health hazards1. Personal protective equipment (PPE) is used to limit exposure to radiation, but because it is heavy and cumbersome, it may also have deleterious health effects2. New light radiation-attenuating materials can efficiently decrease scattered radiation originating from the patient. However, the increasing number and complexity of interventional cardiology procedures require a more global approach to minimise operator exposure to radiation. In collaboration with Lemer Pax, we designed and optimised the Cathpax AIR cabin to improve operator protection during structural procedures and also during coronary angiography and angioplasty. The feasibility of using the cabin during interventional cardiology procedures has been reported previously3. In the present prospective, randomised clinical study performed at Nantes University Hospital (France), we assessed the cabin’s performance regarding radiation protection and ergonomics during structural and coronary angiography/angioplasty procedures (no trial registration exists).
All procedures were randomised daily to be performed with or without the Cathpax AIR cabin (Supplementary Figure 1). The 4 participating interventional cardiologists (P. Guerin, J. Plessis, V. Letocart, and T. Manigold) wore their PPE equipped with thermoluminescent dosimeters for all procedures performed with or without the cabin. The left chest dosimeter provided the total dose received. A cumulative dose was collected over time for both groups of procedures. The primary and secondary endpoints were the differences with and without the cabin in total and individual body part radiation exposure, respectively. Medical team satisfaction with cabin ergonomics was assessed with a questionnaire (Supplementary Figure 2). Additional method description is provided in Supplementary Appendix 1.
This study included 63 structural procedures and 92 angiography/angioplasty procedures performed between March 2021 and January 2022. Patient demographics and procedure characteristics were similar in the groups with and without the cabin (Supplementary Table 1). Use of the cabin reduced the total radiation dose by 63% – from 490 μSv without the cabin (n=31) to 180 μSv with the cabin (n=32) – for the structural procedures, and by 58% – from 810 μSv without the cabin (n=50) to 340 μSv with the cabin (n=42) – for the angiography/angioplasty procedures (Figure 1). The most important benefit provided by the cabin was the protection of the eyes and brain, which had an exposure below the detection limit (<10 μSv) regardless of the procedure (Figure 1). The extremities were also protected by the cabin, with a dose reduction of more than 70% for the left wrist. The questionnaire indicated that cabin installation and physical burden were the major points of dissatisfaction, while accessibility, visibility and communication were satisfactory (Supplementary Figure 3, Supplementary Figure 4).
This study showed an improvement in radiation protection when using the Cathpax AIR cabin during various structural procedures and angiography/angioplasty with no increase in procedure duration or radiation exposure despite some procedures being lengthy and complex. Based on our results, an interventional cardiologist performing 10 structural and 30 angiography/angioplasty procedures per month would receive an annual dose of approximately 3.6 mSv when using the radioprotection cabin, which is below the 5 mSv/year value reported with PPE1. The eyes and brain were particularly protected. This is an advantage of the cabin over radiation protection goggles, which are efficacious4 but not systematically worn because of their weight and the discomfort created. Regarding hand protection, the cabin was superior to PPE, given the lack of reliability of protective gloves5. However, the level of radioprotection reported in this real-life study was not as high as anticipated. Further improvement could be achieved by abandoning the local practice of installing the cabin after performing the vascular approach with fluoroscopic guidance, as was the case for 8 structural procedures. In emergency situations (e.g., external cardiac massage), the cabin would have to be rapidly removed. In that respect, the cabin ergonomics need improvement, as the physical burden associated with cabin handling was described as high. Nevertheless, after set-up, the additional strain induced by the cabin during routine work was acceptable. We did not investigate the safety-related aspects of the cabin, but a review of hospital reports in the early post-intervention phase did not indicate any major complication related to cabin use.
One limitation of our study is the small number of procedures, which, given the low irradiation doses perceived behind the cabin, did not always allow for a precise assessment of benefits. The challenge was to collect a sufficient number of coronary angiography or angioplasty procedures using a cabin, which explains the long inclusion period. Also, the wide range of procedures performed led to significant variability in the use of fluoroscopy, but the study was designed to be representative of daily practice. We evaluated the cabin performance on top of PPE, and an additional study would be necessary to assess the combined radiation protection impact of the cabin and PPE.
In summary, the Cathpax AIR cabin reduces radiation exposure during various routine interventional cardiology procedures. The improvement in radiation protection with the cabin is particularly significant for areas of the body insufficiently protected by standard equipment, such as the skull, the eyes, and the extremities.
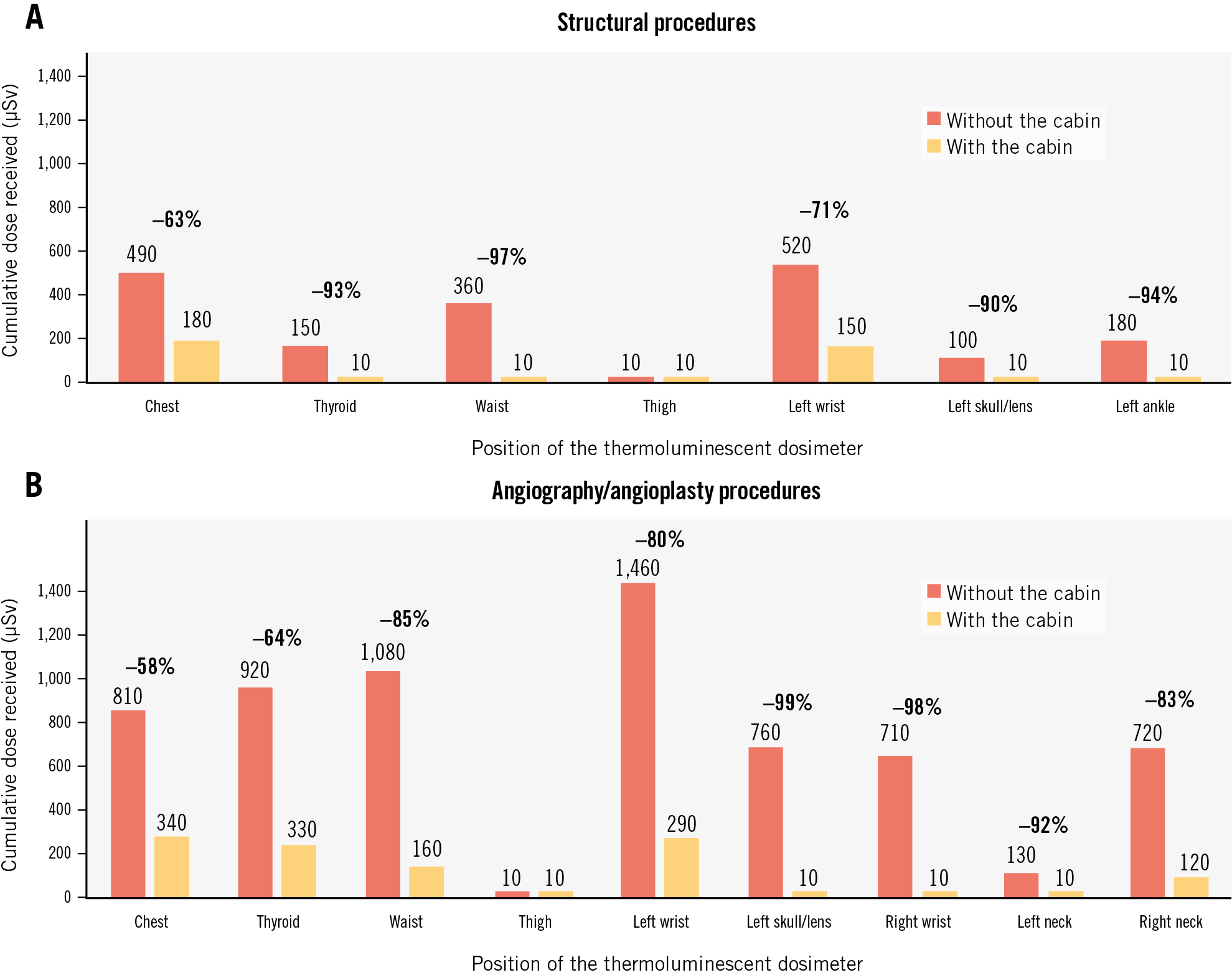
Figure 1. Cumulative dose received by the operator with and without the cabin. Cumulative dose received by the operator during structural (A) and angiography/angioplasty (B) procedures, with and without the radioprotection cabin. The study included 63 structural and 92 coronary angiography/angioplasty procedures. The left chest dosimeter provided the total dose received by the primary operator (study primary endpoint).
Acknowledgements
Thank you to Doctor Virginie Nael, occupational physician, Professor Hatem Necib, radiophysicist at Nantes CHU, and Dr Olivier Bar, interventional cardiologist at the Saint Gatien Clinic, for their contribution to this work and valuable assistance in the field of radiation protection.
Funding
This research did not receive public funding. The prototype of the radioprotection cabin and its improvements were funded by the company Lemer Pax, the owner of the cabin.
Conflict of interest statement
P. Guerin is the initiator of the cabin and has been involved in its creation, design, and optimisation; he has a consultancy agreement with Lemer Pax. The other authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.