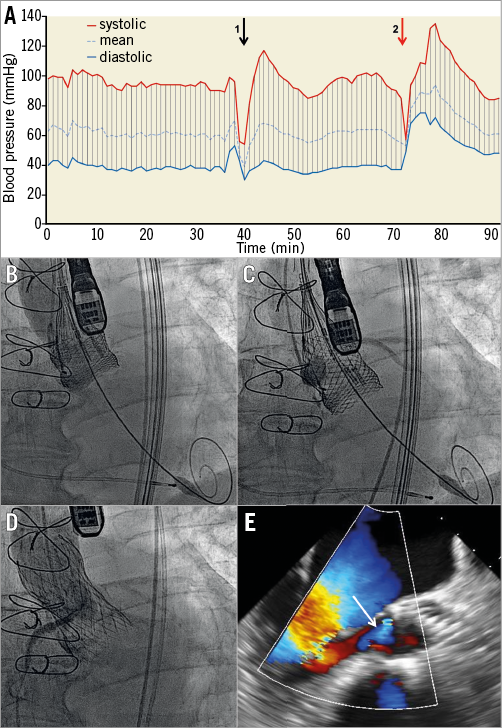
An 80-year-old male patient was admitted to our institution due to new-onset orthopnoea ten years after surgical aortic valve replacement with a 25 mm stentless Freedom Solo bioprosthesis (Sorin Group, Milan, Italy). An echocardiogram revealed severe aortic valve regurgitation owing to a tear in one of the bioprosthetic valve leaflets. In view of the anticipated risk of coronary obstruction associated with this specific type of stentless bioprosthetic valve, TAVI with the use of a fully repositionable 27 mm Lotus™ valve (Boston Scientific, Marlborough, MA, USA) was planned.
Deployment of the Lotus valve was performed aiming at a rather low implantation depth. This led to resolution of the aortic regurgitation. However, immediate haemodynamic compromise (Panel A, arrow point 1) was observed due to the occlusion of both coronary arteries (Panel B). After partial valve retrieval, a contrast injection confirmed restoration of TIMI 3 flow in both coronary arteries resulting in resolution of profound hypotension (Panel A, Panel C, Moving image 1). Repositioning of the Lotus valve at a different depth resulted in a similar haemodynamic compromise due to re-occlusion of the coronary circulation (Moving image 2). As bail-out strategy, a CoreValve® Evolut™ R 29 mm prosthesis (Medtronic, Minneapolis, MN, USA) was successfully deployed (Panel A, arrow point 2). A final aortogram confirmed patency of both coronary arteries (Panel D) with mild paravalvular regurgitation (Panel E, arrow). Furthermore, a sustained rise of the diastolic blood pressure was observed (Panel A).
This report illustrates the value of fully repositionable transcatheter valve prostheses in order to avoid the risk of irreversible coronary obstruction which is increased with some types of surgical stentless bioprostheses.
Conflict of interest statement
T. Pilgrim reports having received research grants to the institution from Biotronik and speaker’s fees from Medtronic and Biotronik. S. Windecker reports receiving research grants to the institution from Abbott, Boston Scientific, Biosensors, Cordis, Medtronic, and St. Jude. The other authors have no conflicts of interest to declare.
Supplementary data
Moving image 1. Restoration of TIMI 3 flow in both coronary arteries after partial valve retrieval.
Moving image 2. Bilateral coronary occlusion despite repositioning of the Lotus valve at a lower depth. Retrieval of the valve.
Supplementary data
To read the full content of this article, please download the PDF.
Restoration of TIMI 3 flow in both coronary arteries after partial valve retrieval
Bilateral coronary occlusion despite repositioning of the Lotus valve at a lower depth. Retrieval of the valve.