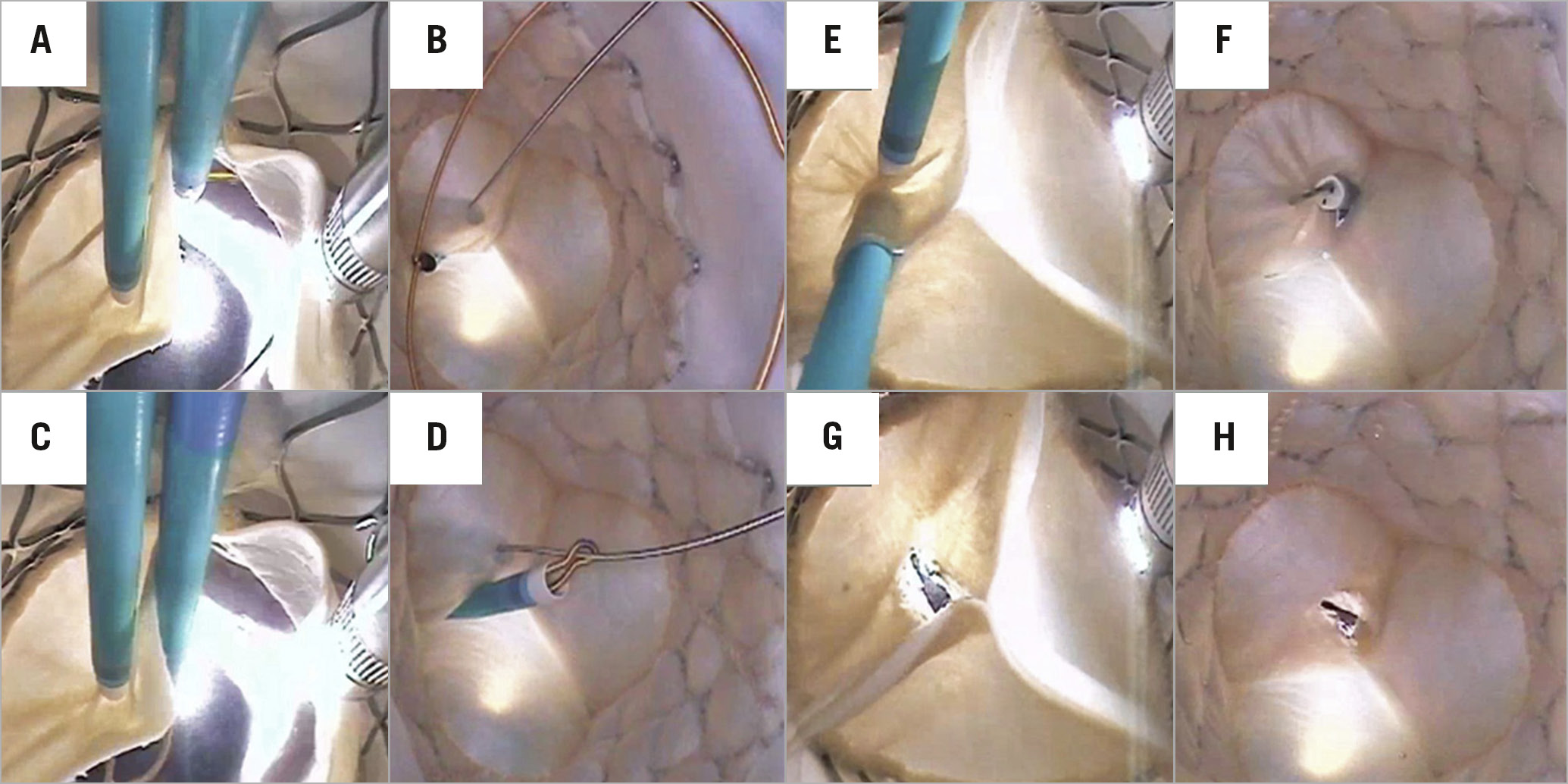
Figure 1. Still images of BASILICA technique procedures recorded from aortic (A,C,E,G) and left ventricular (B,D,F,H) views.
Obstruction of blood flow to the coronary arteries during transcatheter aortic valve replacement (TAVR) is a potentially fatal complication that occurs in ~2.3% of valve-in-valve procedures. Many patients identified at risk of coronary obstruction remain too high a risk for open heart surgery and their treatment is limited to palliative care. In May 2017, a collaboration between the National Institutes of Health (NIH) and the University of Washington developed an electrosurgery catheter-based technique, to slice the leaflets of a failing valve or prosthesis intentionally, so as to increase coronary flow through the displaced leaflets1,2. Bioprosthetic or native Aortic Scallop Intentional Laceration to prevent Iatrogenic Coronary Artery obstruction (BASILICA) has demonstrated feasibility and effectiveness in investigational trials3.
For over two decades, the Visible Heart® Laboratories have utilised a large mammalian ex vivo beating heart preparation to design, test, and develop novel cardiac devices and therapeutic techniques4. Uniquely, we visualised the BASILICA procedure performed by D. Dvir on an implanted 29 mm Evolut™ R (Medtronic, Minneapolis, MN, USA) during TAVR in a reanimated swine heart. Still images of each procedural step were recorded from aortic (Figure 1A, Figure 1C, Figure 1E, Figure 1G) and left ventricular (Figure 1B, Figure 1D, Figure 1F, Figure 1H) views. An electrified guidewire (Astato XS20; Asahi Intecc, Tustin, CA, USA) perforated through the left cusp of the Evolut R and was directed into the open snare positioned in the left ventricular outflow tract (Figure 1A, Figure 1B). The guidewire distal end was captured using snare (ev3 Amplatz Goose Neck™; Medtronic) retrieval (Figure 1C, Figure 1D). The pre-prepared mid-shaft of the guidewire and coronary guide catheter assembly (6 Fr Launcher®; Medtronic) were positioned at the leaflet for laceration (Figure 1E, Figure 1F). An electrosurgical generator (Force FX™; Medtronic) supplied radiofrequency energy of 70W for guidewire perforation and 150W during leaflet laceration. Resulting laceration of the Evolut R prosthesis left cusp allowed the leaflet to splay open (Figure 1G, Figure 1H).
The Visible Heart video of the entire BASILICA procedure and the intentional lacerations within the implanted Evolut R left and right coronary leaflets are provided (Moving image 1). Direct videoscopic visualisation provides educational material for interventional cardiologists aiming to learn and perfect this critical procedure, and industry professionals developing tools to facilitate its clinical application.
Acknowledgements
We wish to acknowledge Dr Michael Bateman and Visible Heart Laboratories staff for their contributions.
Conflict of interest statement
P.A. Iaizzo has a research contract with Medtronic and has received grants from the Institute for Engineering in Medicine (University of Minnesota). D. Dvir is a consultant for Medtronic and Edwards Lifesciences. T. Iles reports other from Medtronic, and grants from the Institute for Engineering in Medicine (University of Minnesota), during the conduct of the study. J. Zhingre Sanchez reports other from Medtronic, and grants from the Institute for Engineering in Medicine (University of Minnesota), during the conduct of the study.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Double-leaflet BASILICA procedure performed in vitro on an Evolut R prosthesis deployed in a reanimated swine heart using Visible Heart methodologies.