Abstract
In patients who have angina with non-obstructive coronary artery disease (ANOCA), invasive coronary function testing (ICFT) is the gold standard to comprehensively diagnose coronary dysfunction. Coronary dysfunction is divided into the endotypes coronary vasospasm, coronary endothelial dysfunction, and coronary microvascular dysfunction (i.e., an abnormal reduced coronary flow reserve [CFR] and/or enhanced microvascular resistance [MR]). However, because of the inherently invasive nature of ICFT, it is important to investigate non-invasive approaches for the diagnosis of coronary dysfunction. Several non-invasive modalities have been proposed as alternative techniques to measure different endotypes of coronary dysfunction. This is promising, given their higher availability and easier applicability. As such, an important clinical question is whether these non-invasive methods are equivalent to invasive tests. In this review, we provide an overview of the invasive and non-invasive diagnostic modalities available to assess coronary dysfunction. Our findings indicate that only CFR can be reliably measured non-invasively, using positron emission tomography (PET), transthoracic Doppler echocardiography (TTDE), and possibly stress cardiac magnetic resonance (CMR) imaging, although the latter has shown conflicting results. Reliable non-invasive techniques to measure coronary vasospasm, coronary endothelial dysfunction, or MR are scarce. Since most patients suffer from more than one coronary dysfunction entity, the added value of non-invasive techniques is still limited. To date, ICFT is the only method capable of investigating all endotypes of coronary dysfunction. Studies investigating the performance of non-invasive modalities for the diagnosis of all components of coronary dysfunction in ANOCA patients are warranted.
Two-thirds of females and one-third of males undergoing a diagnostic coronary angiogram for suspicion of coronary artery disease (CAD) do not have obstructive CAD as an explanation for their symptoms1. The majority (~60-90%) of patients who have angina with non-obstructive coronary artery disease (ANOCA) have coronary dysfunction, which comprises the following endotypes: coronary vasospasm, coronary endothelial dysfunction, and coronary microvascular dysfunction (CMD) (Figure 1)23. Invasive coronary function testing (ICFT) using acetylcholine (ACh) and adenosine is currently the only test that comprehensively assesses all components of coronary function and is recommended in European, Japanese, and American guidelines for diagnosing coronary dysfunction in ANOCA patients4. These patients have an impaired quality of life, higher angina burden and higher incidence of adverse cardiac events25. Identifying the endotypes of coronary dysfunction and subsequently tailoring medical therapy improves quality of life and anginal complaints in these patients6.
ICFT using increasing dosages of intracoronary acetylcholine is used to provoke coronary vasospasm, which encompasses epicardial and/or microvascular coronary vasospasm7. Low-dose (2-20 μg) intracoronary acetylcholine during ICFT is used for the assessment of coronary endothelial dysfunction8. ICFT using adenosine, a non-endothelium-dependent vasodilator, during intracoronary temperature or flow measurement assesses CMD consisting of an abnormal coronary flow reserve (CFR) and/or increased microvascular resistance (MR)9. CMD can be defined as structural (low CFR and high MR) or functional (low CFR and normal/low MR). Despite its diagnostic value, ICFT has several disadvantages compared to non-invasive techniques, including procedural risk (e.g., vascular damage, arrhythmias), higher costs, and greater patient discomfort. Therefore, exploring non-invasive diagnostic modalities and their clinical potential is essential. This review provides an overview of the non-invasive techniques currently available for assessing coronary dysfunction, evaluates their equivalence to ICFT, and discusses their applicability in diagnosing dysfunction in ANOCA patients.
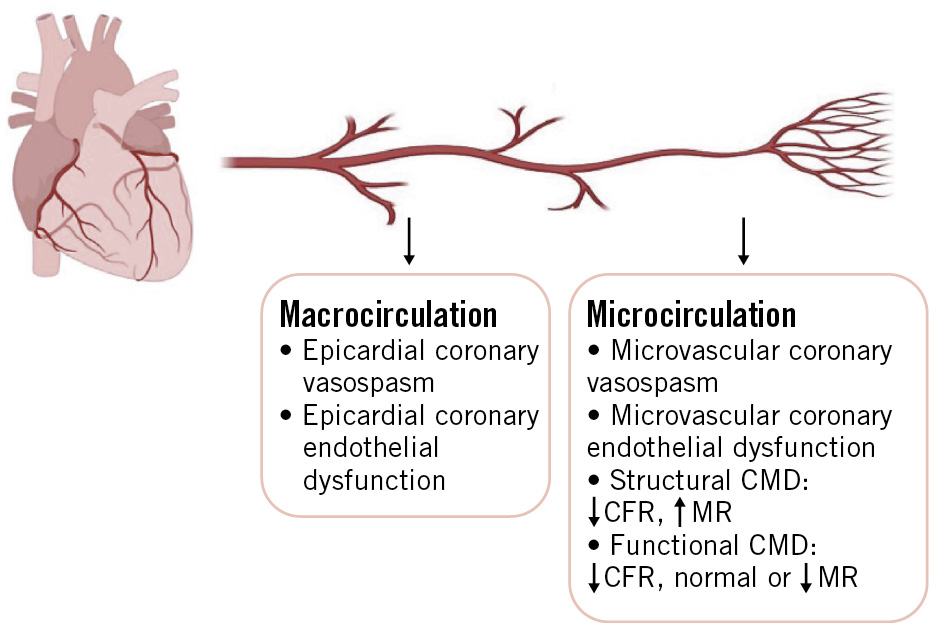
Figure 1. Coronary dysfunction endotypes. Pictograms created with BioRender.com. CFR: coronary flow reserve; CMD: coronary microvascular dysfunction; MR: myocardial resistance
Methods
For this narrative review, we assessed studies published between 2000 and 2022 that compared non-invasive methods for evaluating coronary dysfunction with ICFT in patients with ANOCA (see Supplementary Appendix 1 for the search strategy). Coronary dysfunction includes coronary vasospasm and/or endothelial dysfunction, assessed by ICFT using acetylcholine, and/or abnormal CFR and/or MR, assessed with adenosine. This review focuses specifically on ANOCA; therefore, studies in other clinical contexts (e.g., obstructive CAD or structural heart disease) were excluded. Only patients with stable angina were included; studies involving acute coronary syndromes were not considered.
Techniques, endotypes, and definitions
Assessment of coronary vasospasm
Invasive assessment
ICFT assesses both epicardial and microvascular coronary vasospasm. Although incremental doses of acetylcholine are most often used, other vasoconstrictor agents (e.g., ergonovine, histamine, or serotonin) can also be used10. Acetylcholine is a parasympathetic neurotransmitter that, at high doses (100-200 μg), stimulates endothelial cells to produce vasodilators such as nitric oxide (NO) and also acts directly on vascular smooth muscle cells. Coronary vasospasm is thought to result from hyperreactive smooth muscle cells, either occurring spontaneously or triggered by substances like acetylcholine, combined with endothelial dysfunction, leading to coronary flow limitation11. The COVADIS Group published standardised criteria for diagnosing epicardial and microvascular coronary vasospasm. Epicardial vasospasm requires angina, ischaemic electrocardiogram (ECG) changes, and >90% artery narrowing after acetylcholine. Microvascular vasospasm is defined by angina and ischaemic changes with <90% artery narrowing7 (Table 1).
Table 1. Definitions of the coronary dysfunction endotypes.
| Coronary vasospasm |
|---|
| Epicardial coronary vasospasma |
| Angina symptoms |
| Ischaemic ECG changes either spontaneously or in response to a provocative stimulus (typically ACh [100-200 μg], ergonovine, or hyperventilation) |
| Transient total or subtotal coronary artery occlusion (>90% constriction) |
| Microvascular coronary vasospasma |
| Angina symptoms |
| Ischaemic ECG changes either spontaneously or in response to a provocative stimulus (typically ACh [100-200 μg], ergonovine, or hyperventilation) |
| Absence of total or subtotal coronary artery occlusion (<90% constriction) |
| Coronary endothelial dysfunction |
| Epicardial coronary endothelial dysfunction |
| Epicardial minimal lumen diameter constriction of >0% or >20% during low-dose intracoronary ACh reactivity testing (ACh dosage 20 μg) |
| Microvascular coronary endothelial dysfunction* |
| Increase in volumetric coronary blood flow of ≤50% during low-dose intracoronary ACh reactivity testing (ACh dosage 20 μg) |
| Coronary microvascular dysfunction |
| Impaired coronary flow reserve |
| Hyperaemic APV divided by APV at rest. Depending on the methodology used, CFR is considered abnormal when ≤2.0 or ≤2.5 |
| Increased microvascular resistance |
| Hyperaemic microvascular resistance: the ratio of hyperaemic mean distal pressure to hyperaemic APV. An HMR >2.5 is considered abnormal* |
| Index of microvascular resistance: multiply the hyperaemic mean distal pressure by the hyperaemic mean transit time. An IMR >25 is considered abnormal |
| Structural CMD |
| Impaired CFR |
| Increased MR |
| Functional CMD |
| Impaired CFR |
| Normal/low MR |
| aCoronary vasospasm (epicardial or microvascular) is only diagnosed if all three criteria are present. *ComboWire (Philips Volcano), used for intracoronary flow measurements, is required for the assessment. ACh: acetylcholine; APV: average peak velocity; CFR: coronary flow reserve; CMD: coronary microvascular dysfunction; ECG: electrocardiography; HMR: hyperaemic MR; MR: microvascular resistance |
Non-invasive assessment
To date, hyperventilation in combination with the cold pressor test (CPT) has been described as a clinical tool to non-invasively induce coronary vasospasm12. Hyperventilation activates the sympathetic nervous system, leading to an increased release of catecholamines and provoking vasoconstriction. This heightened vasoconstrictive activity can outweigh the vasodilator influence of NO in individuals with endothelial dysfunction, contributing to the occurrence of coronary vasospasm13. During the hyperventilation provocation test, a 12-lead ECG is continuously monitored while patients are instructed to hyperventilate for 6 minutes. If recognisable chest pain occurs and/or ST-segment elevation appears on the ECG during hyperventilation, the test is considered positive for coronary vasospasm.
Comparing non-invasive and invasive diagnostic modalities
Only 2 studies comparing ICFT using acetylcholine with a non-invasive method were found. One study by Hirano et al (2001) compared ICFT using acetylcholine with hyperventilation cold-pressor stress echocardiography in 43 patients (56±10 years, 37% females) with suspected vasospastic angina14. The study combined hyperventilation and the CPT by submerging the patient’s right hand in iced water for 2 minutes after hyperventilation for 6 minutes. Coronary vasospasm was observed in 33 patients by angiography and in 26 patients with stress echocardiography. This resulted in a diagnostic accuracy of 91%, sensitivity of 90%, and specificity of 91%. However, this non-invasive technique is unable to differentiate between epicardial and microvascular vasospasm, which is crucial for providing tailored treatment. Furthermore, implementing the combination of hyperventilation and CPT in a clinical setting is challenging due to the significant discomfort and pain it causes for the patient.
One study compared ICFT using acetylcholine, for coronary vasospasm diagnosis, with stress cardiac magnetic resonance (CMR) imaging, in 129 patients (65 years old, 53% females)15. Stress CMR imaging was used to determine the myocardial perfusion reserve index (MPRI), the ratio of myocardial blood flow (MBF) at stress over MBF at rest. Hyperaemia was induced by intravenous administration of adenosine (140 μg/kg/min). The study population was divided into three groups: (1) epicardial coronary vasospasm (n=29, 41% females), (2) microvascular coronary vasospasm (n=69, 67% females), and (3) no coronary vasospasm (n=31, 32% females). Overall, patients with epicardial coronary vasospasm had a significantly lower MPRI compared to patients without (1.15±0.24 vs 1.41±0.25; p<0.001); however, in patients with microvascular coronary vasospasm, the MPRI did not differ from that of patients without microvascular coronary vasospasm. Although patients with epicardial coronary vasospasm had a significantly lower MPRI compared to patients without, comparing the endothelium-independent stressor adenosine with the invasively measured coronary vasospasm (i.e., presence of epicardial constriction, ECG changes, and angina complaints) that is induced by the endothelium-dependent vasodilator acetylcholine seems unreliable. Endothelium-dependent and -independent vasodilation involve different pathophysiological mechanisms, complicating comparisons. The significant outcome could be explained by overlapping endotypes in patients with coronary dysfunction. Patients with epicardial vasospasm had significantly more CAD, which is associated with lower CFR and may explain the result. However, CFR was not measured in these patients. To date, there are no reliable non-invasive modalities for accurately assessing coronary vasospasm and the contribution of epicardial versus microvascular vasospasm in the clinical setting.
Assessment of coronary endothelial dysfunction
Invasive assessment
Coronary endothelial dysfunction is assessed by ICFT using low-dose acetylcholine, most commonly through 3-minute infusions. At low dosages (2-20 μg), acetylcholine primarily acts on the endothelium, causing vasodilation in healthy vessels via NO production. In endothelial dysfunction, the endothelium fails to respond adequately to acetylcholine by producing NO, resulting in impaired vasodilation. Epicardial endothelial dysfunction is most commonly defined as constriction of>0% or >20% of the minimal lumen diameter (MLD) of the epicardial vessels after administration of low-dose acetylcholine compared to baseline diameter. Microvascular endothelial dysfunction is defined as an increase in volumetric CBF of <50%23 (Table 1). A ComboWire (ComboWire XT [Philips Volcano]) is used for simultaneous measurement of coronary pressure and flow through which the average peak velocity (APV) is calculated16.
Non-invasive assessment
A non-invasive method to assess coronary endothelial dysfunction is the CPT. This test uses an external cold stimulus, for example, by wrapping an ice pack around a hand or forearm or immersing a hand in cold water between 0-5 degrees for +/- 2 minutes1718. This causes an increase of coronary shear stress, which leads to endothelium-dependent flow-mediated vasodilatation by production of NO in case of an intact endothelium18. This effect is comparable with the effect of low-dose ACh on the endothelium23. In healthy coronary arteries, the physiological response to CPT is vasodilation; however, when coronary endothelial dysfunction is present, vasoconstriction of the arteries occurs. CPT is often combined with CMR imaging or positron emission tomography (PET)19.
A potential new, useful, non-invasive technique is flow-mediated dilation, which assesses peripheral endothelial function and may indirectly reflect coronary health. Similarly, assessing peripheral vascular smooth muscle cells with laser speckle contrast analysis (LASCA) technology shows promise for detecting coronary dysfunction. Both methods offer less invasive alternatives to coronary testing, but further research is needed to confirm their clinical value2021.
Comparing non-invasive and invasive diagnostic modalities
Three studies compared invasive and non-invasive modalities for diagnosing coronary endothelial dysfunction. However, only one study by Landes et al17 compared ICFT using acetylcholine with the CPT in combination with the MPRI. The study population consisted of 189 females (54±11 years old) with ANOCA. Despite the fact that the acetylcholine provocation test and the CPT both induce endothelium-dependent vasodilation, no correlation was found. This may be explained by differences in outcome measures. The MPRI is a semiquantitative ratio of stress-to-rest perfusion upslopes, whereas intracoronary acetylcholine testing uses changes in coronary diameter and coronary blood flow (CBF). Furthermore, CPT cannot distinguish between coronary microvascular and epicardial endothelial dysfunction, and it is challenging to perform in clinical practice.
Thomson et al (2015)22 investigated the relationship between coronary endothelial dysfunction measured by ICFT with low-dose acetylcholine and MPRI in 118 females (54±11 years old). For the MPRI, stress was induced by adenosine. A correlation was found between MPRI and epicardial endothelial dysfunction (R=0.22; p=0.029), as well as for microvascular endothelial dysfunction (R=0.29; p=0.005). However, both techniques measure different vasodilator pathways (i.e., endothelium-dependent and -independent vasodilatation), which limits the interpretation by direct comparison.
Finally, Pargaonkar et al23 investigated the relationship between ICFT using low-dose acetylcholine and non-invasive stress echocardiography and ECG in 155 patients (54 years old, 76.7% females). In this study, only epicardial endothelial dysfunction was investigated. Stress was induced by exercise or administration of dobutamine. Patients diagnosed with epicardial endothelial dysfunction via ICFT did not exhibit a higher incidence of positive stress echocardiography results compared to those without this condition (p=0.19). Stress ECG was associated with the presence of coronary endothelial dysfunction in females (p=0.03) but not in males.
Assessment of coronary microvascular dysfunction by CFR
Invasive assessment
CFR, used to diagnose CMD, can be measured invasively via Doppler or thermodilution. A Doppler wire (e.g., ComboWire XT) assesses flow velocity and calculates CFR as the ratio of hyperaemic to resting APV. Hyperaemia can be induced by either intravenous or intracoronary administration of adenosine. Recent studies have demonstrated no significant differences between the two techniques24. In ANOCA patients, CFR <2.0 is abnormal, >2.5 is normal, and 2.0-2.5 represents a borderline zone16. The thermodilution technique uses a pressure-temperature guidewire (e.g., PressureWireX Guidewire [Abbott]) to assess coronary flow indirectly by measuring the average mean transit time of a room temperature bolus of intracoronary saline. The mean transit times at rest and during hyperaemia are measured, and subsequently, CFR is calculated as the ratio of the hyperaemic to resting mean transit time25 (Table 1).
Non-invasive assessment
Several non-invasive alternatives exist to assess CFR. The non-invasive gold standard is PET-derived CFR26, but transthoracic Doppler echocardiography (TTDE) and stress CMR imaging can also be used27. For all non-invasive methods, the same cutoff value of 2.0 was used.
The gold standard for non-invasive assessment of MBF and CFR is PET using oxygen-15-labelled water (150H20-PET). PET is a radionuclide imaging technique which quantifies myocardial perfusion. For CFR measurements, the MBF is calculated at rest and during (maximal) hyperaemia, after infusion of pharmacological endothelium-independent vasodilators (most commonly adenosine)28.
TTDE measures coronary flow velocity reserve (CFVR) in the (mid-distal) left anterior descending coronary artery (LAD). A high-frequency probe with a modified 2- or 4-chamber view and colour Doppler flow mapping guidance is used to locate the LAD. After baseline measurements at rest, a vasodilator stressor such as adenosine or dobutamine is administered to induce maximal hyperaemia with repeated measurements29.
CMR can quantify absolute MBF in mL/min/g during rest and stress conditions (after administration of a pharmacological vasodilator, typically adenosine or ergonovine). The potential of CMR for non-invasive assessment of CMD by CFR measurement was demonstrated decades ago in early studies, such as that by Panting et al30. Both myocardial perfusion reserve (MPR) and MPRI represent the ratio of MBF between stress and rest, but they are calculated using different methods31. MPR and MPRI can be considered surrogates for CFR32. Figure 2 provides an overview of the advantages and disadvantages of the non-invasive diagnostic modalities for CMD.
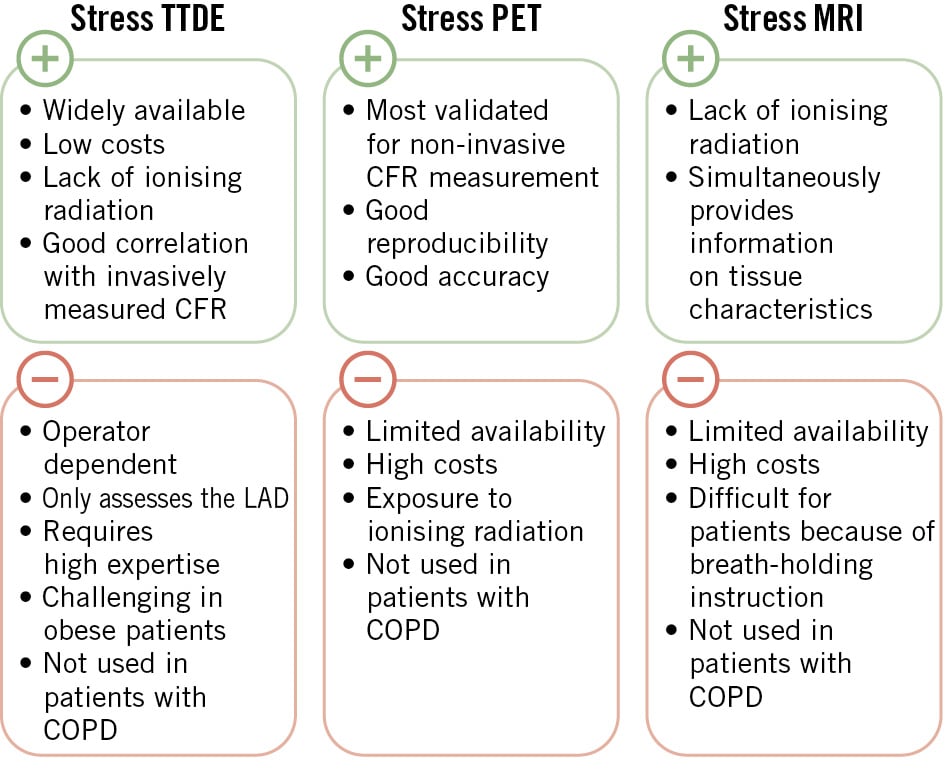
Figure 2. Non-invasive techniques for coronary microvascular dysfunction. CFR: coronary flow reserve; COPD: chronic obstructive pulmonary disease; LAD: left anterior descending artery; MRI: magnetic resonance imaging; PET: positron emission tomography; TTDE: transthoracic Doppler echocardiography
Comparing non-invasive and invasive diagnostic modalities
Non-invasive measurements of CFR for the diagnosis of CMD seems promising, especially using TTDE and PET. Although there are no clinical studies to confirm this in ANOCA patients, the gold standard for CFR measurements is PET. This technique has demonstrated an excellent correlation with invasive CFR, predominantly when the Doppler wire is used during ICFT26. Although this method is considered the gold standard for non-invasive assessment of myocardial blood flow and CFR, it has limitations due to the use of radiation and the high costs and is therefore not widely available.
Three small prospective studies (consisting of 51 [55±11 years old, 41% females], 17 [65% females] and 37 [54±12 years old, 41% females] participants, respectively) compared TTDE CFVR with invasive CFR measured using the Doppler technique333435. These studies reported an excellent correlation between TTDE CFVR and invasive CFR (R coefficient and p-value: R=0.87; p<0.00133; R=0.72; p<0.0134; R=0.88; p<0.00135, respectively). The success rates for the assessment of CFVR in the LAD were 98%, 81%, and 93%, respectively, indicating that it is a promising non-invasive technique for the evaluation of CFR. This may be explained by the similarities between the two methods. Both methods measure the ratio between rest and hyperaemic flow velocity using adenosine. Although this technique is cheap, extensive training is required to perform it reliably. Moreover, it is not suitable for all patients, as image quality may be poor due to patient habitus29.
Three studies investigated the correlation between CMR and invasively assessed CFR. First, the study by Thomson et al22 reported no correlation between MPRI and invasive CFR (R=0.16; p=0.08), among 118 females (54±11 years old) with ANOCA. Second, the study by Rahman et al (2019)36 found that patients (n=85, 57±10 years old, 78% females) with invasively measured abnormal CFR had a significantly lower MPR (p<0.001) and higher resting MBF (p=0.004) compared to patients with normal CFR. Third, another article published by Rahman et al37 investigated the diagnostic accuracy of MPR to predict an abnormal response to the ICFT (n=75 patients, 57±10 years old, 81% females). They reported that an MPR threshold of 2.19 showed excellent specificity for detecting abnormal CFR as measured by Doppler using adenosine (abnormal CFR defined as <2.5).
Additionally, recent frameworks distinguish functional CMD (reduced CFR, normal IMR) from structural CMD (reduced CFR and increased IMR), a distinction only made possible with invasive assessment measuring both CFR and IMR. Although CFR can be measured non-invasively, no validated non-invasive method exists for IMR. Thus, non-invasive diagnostics cannot currently differentiate between functional and structural CMD.
Assessment of coronary microvascular dysfunction by microvascular resistance
Invasive assessment
The Doppler technique determines hyperaemic microvascular resistance (HMR) by calculating the ratio of hyperaemic mean distal pressure to hyperaemic APV. An HMR >2.5 is most commonly used as the cutoff value for an abnormal HMR. The thermodilution technique assesses the IMR by measuring the mean transit times, which have been explained previously. The IMR is calculated by multiplying the hyperaemic mean distal pressure by the hyperaemic mean transit time. An IMR >25 is considered abnormal38 (Table 1).
Intermediate invasive assessment
The angiography-derived IMR (angio-IMR) enables wire- and drug-free assessment of MR using standard coronary angiography and computational flow dynamics. By estimating distal pressure and hyperaemic flow from contrast data, angio-IMR provides a fully invasive alternative to traditional IMR, with values >25 indicating abnormal resistance. Recent studies support its feasibility and accuracy in patients with suspected ANOCA, highlighting its potential clinical utility39. This technique is considered intermediately invasive because it uses data from invasive coronary angiography but does not require additional instrumentation or pharmacological hyperaemia. The IMR can be calculated retrospectively from high-quality angiographic images.
Non-invasive assessment
To date, no non-invasive diagnostic modality is available to assess MR, although studies described below compare non-invasive modalities with invasive MR assessment. However, these techniques are still insufficient for determining MR, which requires simultaneous pressure measurement, and are typically used for CFR measurements (as described above).
Comparing non-invasive and invasive diagnostic modalities
Two studies compared invasive IMR with a non-invasive diagnostic modality. First, Kotecha et al (2019) investigated the relationship between IMR and CMR40 in 23 ANOCA patients (64±8 years old, 35% females), 27 patients with obstructive CAD (62±9 years old, 7% females), and 15 healthy controls (45±8 years old, 13% females). For ANOCA patients, this study found that global stress MBF measured by CMR was significantly lower in vessels with an IMR >25 compared to vessels with an IMR <25 (p=0.004). Second, Pargaonkar et al (2019), investigated the ability of stress echocardiography and ECG to identify IMR non-invasively23. Stress was induced by exercise or administration of dobutamine and considered positive when wall motion abnormalities occurred. In patients with an abnormal IMR, there was no significant difference in the frequency of positive TTDE results or ischaemic ECG findings compared to those with a normal IMR.
The proposed non-invasive techniques for measuring MR do not assess the same variables as the invasive techniques. MR is the ratio between distal coronary pressure and hyperaemic flow, while the proposed non-invasive technique based on MPRI calculates the ratio between resting and hyperaemic MBF (and does not include pressure measurements). Myocardial resistance reserve is a promising invasive index for solely evaluating microvascular function, using continuous thermodilution without bolus injections. While not yet validated against non-invasive imaging, it underscores the importance and value of invasive testing. Another interesting study by Sinha et al (2024) showed that ECG ischaemia during exercise stress testing (EST) had 100% specificity for invasive CMD markers in ANOCA, challenging prior assumptions about EST’s diagnostic accuracy41.
Supplementary Table 1 and the Central illustration both provide overviews of all the available diagnostic modalities, with the corresponding advantages and disadvantages. An overview of the studies that compared non-invasive and invasive diagnostic modalities for the diagnosis of coronary dysfunction and the outcomes of these studies are presented in Supplementary Table 2.
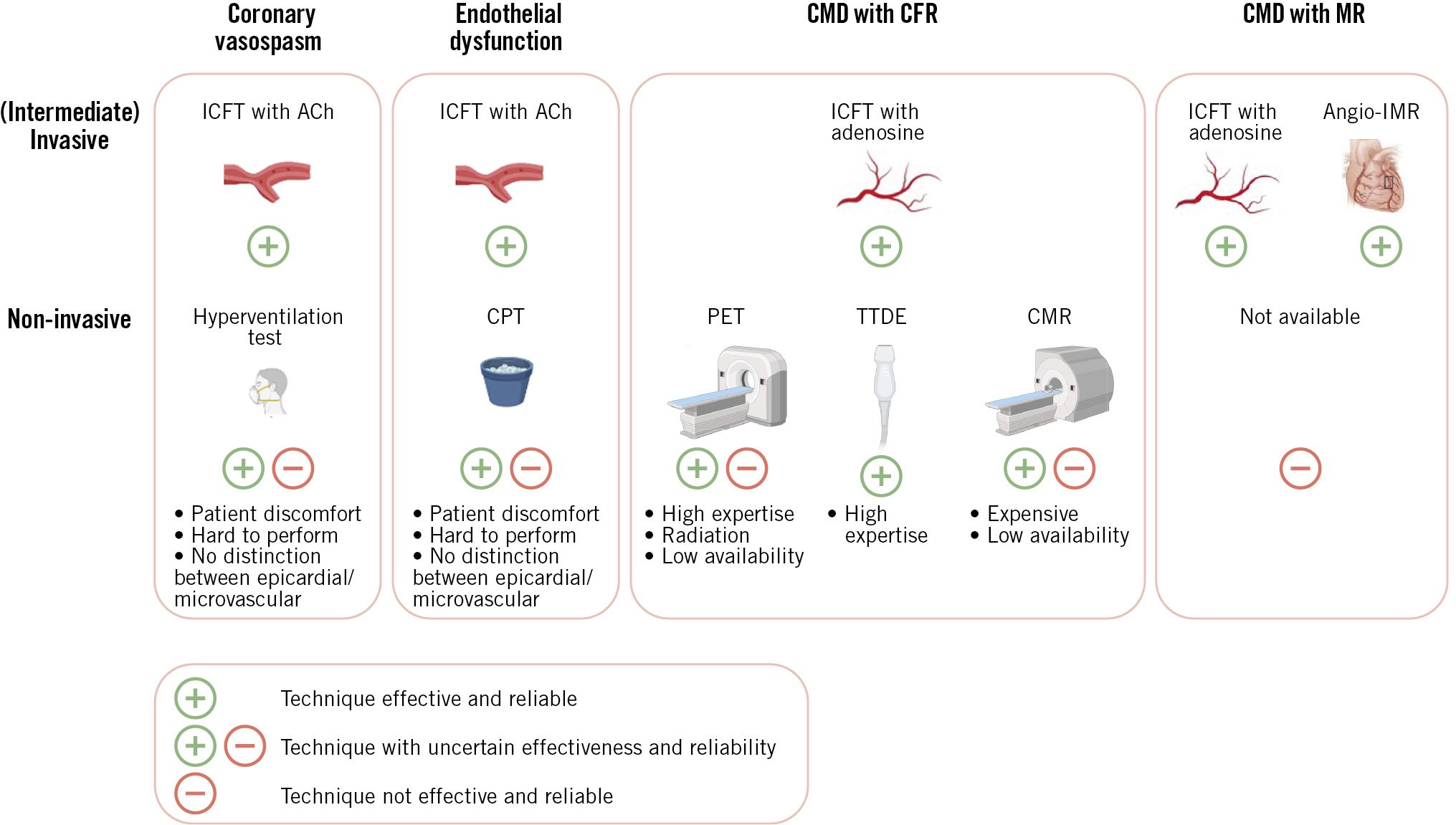
Central illustration. Non-invasive versus invasive techniques for coronary dysfunction. Pictograms created with BioRender.com. ACh: acetylcholine; angio-IMR: angiography-derived index of microvascular resistance; CFR: coronary flow reserve; CMD: coronary microvascular dysfunction; CMR: cardiac magnetic resonance; CPT: cold pressor test; ICFT: invasive coronary function test; MR: myocardial resistance; PET: positron emission tomography; TTDE: transthoracic Doppler echocardiography
Clinical implications
A relatively high correlation was found between invasive CFR and non-invasive CFR with PET and TTDE, while for the other endotypes of coronary dysfunction the non-invasive techniques showed varying or unreliable results. Most patients with coronary dysfunction suffer from coronary vasospasm or coronary endothelial dysfunction, with or without an impaired CFR or MR6. This review provides evidence that the most common endotype of coronary dysfunction (coronary vasospasm) cannot be effectively measured non-invasively. Furthermore, many patients suffer from a combination of the different coronary dysfunction endotypes. Thus, to date, no non-invasive diagnostic modality can assess all aspects of coronary dysfunction, and extensive invasive coronary function testing is needed to provide the patient with a diagnosis and tailored treatment.
Conclusions
To our knowledge, this is the first review to provide an overview of studies comparing invasive and non-invasive diagnostic modalities available for evaluating coronary dysfunction. To date, non-invasive methods cannot capture all endotypes of coronary dysfunction (i.e., coronary vasospasm and coronary endothelial dysfunction), and ICFT remains the gold standard for the assessment of coronary dysfunction in ANOCA patients. Large, well-designed, prospective studies investigating the diagnostic accordance between the currently available non-invasive and invasive modalities in both male and female ANOCA patients are warranted. Additionally, future studies are needed to explore non-invasive modalities capable of diagnosing all components of coronary dysfunction, especially those focusing on coronary vasospasm and endothelial dysfunction. However, in order to diagnose and treat patients with ANOCA, invasive physiological measurements are indispensable and should be in the armamentarium of every interventional cardiologist.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.