Renal artery stenosis may cause or deteriorate arterial hypertension and/or renal insufficiency. Technical improvements of diagnostic and interventional endovascular tools have led to a more widespread use of endoluminal renal artery revascularisation and extension of the indications for this type of therapy. The first renal artery balloon angioplasties were performed by Felix Mahler in Berne and Andreas Gruentzig in Zurich in 19771,2. Until the beginning of the 1990’s balloon angioplasty was the only method of percutaneous treatment of renal artery stenosis (RAS). Results were satisfying for stenoses caused by fibro-muscular dysplasia and atherosclerotic stenosis of the renal artery trunk, but limited for ostial atherosclerotic lesions, the most common manifestation of renal artery stenosis3,4. The introduction of stenting has revolutionised percutaneous renal revascularisation. Following promising single centre reports, two randomised studies proved the superiority of stenting over conventional balloon angioplasty3,5 in the treatment of atherosclerotic ostial renal artery stenosis. Nowadays using pre-mounted low profile stent devices atherosclerotic RAS can be treated successfully in almost all cases with restenosis rates ranging from 0 to 23% depending on the diameter of the renal artery5-9. Even if the recent randomised STAR and ASTRAL trials10,11 did not show any benefit of renal artery stenosis revascularisation over medical therapy there is nonetheless evidence that stenting of haemodynamically relevant atherosclerotic renal artery stenosis has an impact on blood pressure control, renal function, and left ventricular hypertrophy. A proper patient selection and a safe interventional technique are the key elements of a clinically successful outcome of the patient following the procedure. In particular, patients with a short history of deterioration of renal function might have the largest benefit from intervention. In patients with an advanced stage of renal failure the indication for stenting of atherosclerotic renal artery stenosis must be determined individually for each patient considering the overall prognosis. The online version of this manuscript introduces step-by-step into interventional treatment techniques for renal artery stenoses, from the simple guiding catheter technique to the modified “no-touch” technique (Figure 1a-e) or the telescope technique to access renal arteries with steep angulations from the femoral artery.
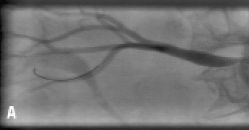
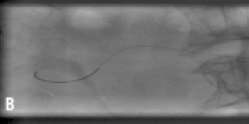
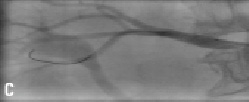

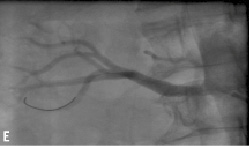
Figure 1. Stenting of right renal artery using a modified “no-touch” technique: a) Severe right RAS b) One 0.014” wire each in the renal artery and the suprarenal aorta c) Placement of the stent. d) Release of the stent, aortic wire still in place e) Final result.
