Cory:
Unlock Your AI Assistant Now!
Multiple coronary protection strategies have been described to reduce the risk of coronary obstruction during redo-transcatheter aortic valve implantation (redo-TAVI). However, their effectiveness can be limited by anatomical or valve-related factors12. The Undermining Iatrogenic Coronary Obstruction with Radiofrequency Needle (UNICORN) leaflet modification technique offers a potentially attractive approach during redo-TAVI, as it allows for greater clearance of the obstructing leaflet3. Nonetheless, we highlight an important consideration regarding the safety and efficacy of the UNICORN technique in this context.
A 78-year-old male was planned for redo-TAVI to address a severely regurgitant and degenerated ACURATE neo2 valve (ACn2; Boston Scientific). Preprocedural computed tomography (CT) revealed the left coronary artery (LCA) to be at high risk for coronary obstruction, with the neoskirt plane for a SAPIEN 3 (S3; Edwards Lifesciences) extending above the coronary risk plane and a valve-to-aorta distance of less than 2 mm. Given the good commissural alignment of the index ACn2, leaflet modification with UNICORN was planned to mitigate the risk of coronary obstruction.
The procedure involved using a 7 Fr Amplatz left (AL) 3 guide catheter, a FineCross microcatheter (Terumo), and an Astato XS 40 0.014” wire (Asahi Intecc) energised at 50W to perforate the leaflet facing the LCA (Figure 1A). Sequential balloon dilatations (3.5 mm, 5 mm, 8 mm, and 14 mm) were performed to enlarge the puncture site sufficiently to facilitate S3 crossing. Immediately after inflating the 14 mm balloon, the patient developed haemodynamic instability due to massive aortic regurgitation, necessitating rapid deployment of the S3 valve. The S3 was successfully implanted at the intended position – the S3 outflow aligned with the upper crown of the ACn2 − resulting in good haemodynamic valve performance and preserved LCA patency (Moving image 1).
Post-implant CT confirmed correct S3 positioning, with residual partial leaflet overhang of the right and non-coronary leaflets of the ACn2. An irregularly shaped, highly mobile avulsed left coronary leaflet was also observed attached to the ACn2 commissural post (Figure 1B). To better understand this phenomenon, patient-specific bench testing was performed to replicate the redo-TAVI procedure and various UNICORN scenarios. An internally mounted borescope provided real-time observation of the UNICORN-treated leaflet (Figure 1C).
The tests revealed that if leaflet avulsion occurred prior to S3 implantation, the highly mobile leaflet risked being displaced towards the target sinus and being trapped between the valve frames. This could potentially compromise coronary flow and access, negating the benefits of the UNICORN technique (Moving image 2). Conversely, if avulsion was avoided before deploying the S3, and instead the subsequent S3 inflation was used to avulse the leaflet, the target leaflet was displaced towards the opposite side in a more consistent and controlled manner. This approach maximised sinus clearance and minimised the risk of coronary obstruction (Moving image 3).
These findings underscore the need for caution when employing the UNICORN technique during redo-TAVI. Sufficient predilatation of the target leaflet is necessary to facilitate passage of the second valve, but it must be balanced against the risks associated with complete avulsion. However, determining the precise timing and balloon size required for complete leaflet avulsion is unpredictable. Loss of the balloon waist during leaflet predilatation, accompanied by centralisation of the balloon and a sudden drop in blood pressure, should alert operators to the possibility that complete leaflet avulsion has occurred.
If complete leaflet avulsion is suspected, then following valve implantation, orthotopic coronary wiring and stenting can be performed to mitigate the risk of coronary obstruction by the unpredictable leaflet motion. This may be of particular benefit in scenarios where complete leaflet avulsion is preferred, such as if revalving with a self-expanding platform. Further research is essential to optimise the safety and predictability of the UNICORN procedure.
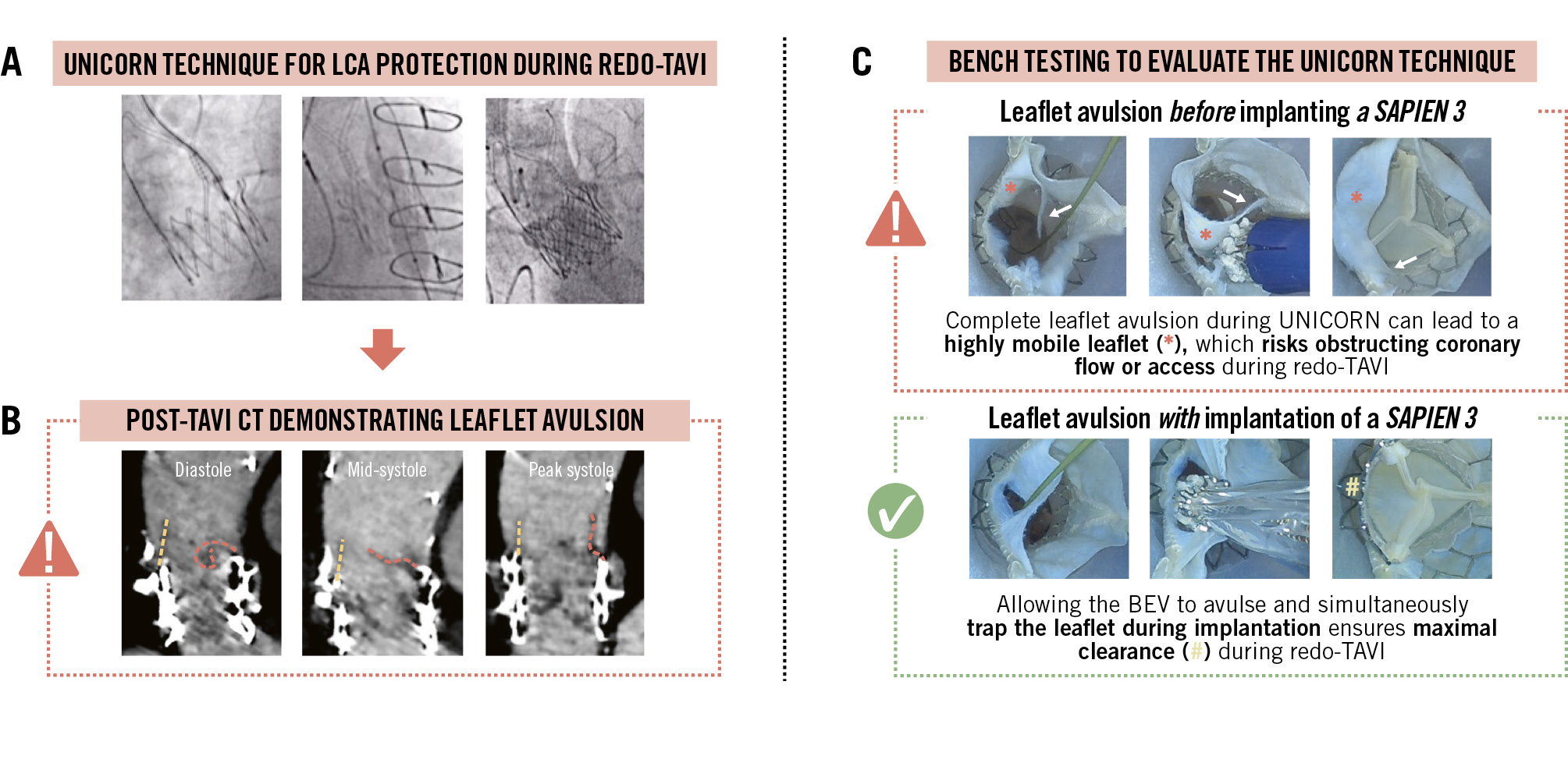
Figure 1. Leaflet dynamics following UNICORN leaflet modification to overcome coronary obstruction during redo-TAVI. A) Redo-TAVI with a SAPIEN 3 (S3) was utilised to treat a degenerated ACURATE neo2 (ACn2) transcatheter aortic valve. The risk of obstruction to the left coronary artery (LCA) was deemed high, and therefore, leaflet modification with the UNICORN technique was performed prior to S3 implantation. B) Post-implantation computed tomography (CT) demonstrated leaflet overhang (dashed yellow line) and an irregular-shaped avulsed leaflet (dashed red line), which was highly mobile throughout the cardiac cycle. C) Patient-specific bench testing was performed to observe leaflet behaviour following different UNICORN strategies: complete leaflet avulsion prior to S3 implantation increased the risk of compromising coronary access and coronary obstruction. BEV: balloon-expandable valve; TAVI: transcatheter aortic valve implantation; UNICORN: Undermining Iatrogenic Coronary Obstruction with Radiofrequency Needle
Acknowledgements
The authors would like to acknowledge Conor White, Jochem van der Kooij, and the rest of the team at the Simulation Lab in Galway, Ireland.
Conflict of interest statement
A.A. Khokhar received speaker/honoraria fees from Abbott, Boston Scientific, and Medtronic. A. Beneduce received speaker fees from Boston Scientific. Y. Kobari has received speaker fees from Abbott and Boston Scientific. G. Bieliauskas has received speaker honoraria and consulting fees from Abbott, Boston Scientific, Edwards Lifesciences, Medtronic, and Sahajanand Medical Technologies Ltd. O. De Backer received institutional research grants and consulting fees from Abbott, Boston Scientific, and Medtronic.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. UNICORN-assisted redo-TAVI with SAPIEN-in-ACURATE neo2.
Moving image 2. Leaflet avulsion before SAPIEN 3 implantation.
Moving image 3. Leaflet avulsion during SAPIEN 3 implantation.