Cory:
Unlock Your AI Assistant Now!
Several algorithms have been proposed to address the issue of uncrossability and impenetrability; however, these challenges remain a significant cause of failure in percutaneous coronary intervention (PCI) procedures1234.
We describe an alternative technique to enhance support and penetration safely and efficiently: the Anchor the Mother to Advance the Child (AMAC) technique. This approach successfully facilitated a multiattempt, complex coronary total occlusion (CTO) PCI, where all other options had failed.
A 58-year-old male with a long-standing, calcific CTO of the right coronary artery (Figure 1A, Moving image 1) was admitted to our hospital due to unresponsive angina despite medical therapy. The CTO had been previously documented, and the patient had undergone three unsuccessful treatment attempts by experienced operators. These attempts failed because the midsection of the occlusion was uncrossable, and the distal part was impenetrable (Supplementary Figure 1). After a collegial discussion, we decided to make one final attempt at treatment.
The right coronary artery was engaged using an 8 French (Fr) Amplatz Left (AL) 1 catheter through the right femoral artery. At the same time, the left system was accessed with a 7 Fr extra-backup catheter from the right radial artery.
During this procedure, we encountered an uncrossable lesion in the midsection, which was not penetrable retrogradely in the distal part. Additionally, attempts at subintimal tracking to cross the lesion were unsuccessful, and a small perforation occurred during a deliberate balloon rupture (grenadoplasty) manoeuvre. As a result, we decided to pursue an unconventional approach.
First, we attempted the Anchor-Tornus technique, using a 2.5x12 mm anchor balloon placed within the conus branch along with a screwable microcatheter positioned in the proximal cap. Unfortunately, this attempt was not successful (Supplementary Figure 2).
Next, while keeping the anchor balloon in place, we advanced a 5 Fr guide extension anterogradely within the same guide catheter adjacent to the balloon, employing the AMAC technique. For the first time throughout all the procedures, this manoeuvre allowed us to cross the midsection of the occlusion successfully, enabling the guide extension to be positioned distally in an inchworm fashion (Figure 1B-Figure 1C-Figure 1D-Figure 1E, Moving image 2, Supplementary Figure 3). This position provided optimal support for accessing the distal part using a directional wire, which was aided by a screwable microcatheter to cross the lesion in an intraplaque manner, referred to as the Modified Anchor-Tornus Technique (Figure 1C-Figure 1D-Figure 1E-Figure 1F, Moving image 3, Supplementary Figure 3). A retrograde marker wire was introduced into the crux, serving as a marker for the kissing wire technique. Once the intraluminal position of the wire in the posterolateral branch was confirmed, a small-profile microcatheter could only be advanced after performing another grenadoplasty at the level of the distal cap. Eventually, the CTO was successfully crossed.
Superhigh-pressure balloons (40 atm) and multiple lithotripsy cycles were utilised to prepare the lesion. Ultimately, the artery was treated using a “leaving nothing behind” approach with sirolimus-eluting drug-coated balloons (Figure 1D, Moving image 4).
The AMAC technique is an alternative to enhance support and improve crossability and penetrability in complex PCI. This manoeuvre should be included in the algorithmic strategy for addressing uncrossable and impenetrable lesions.
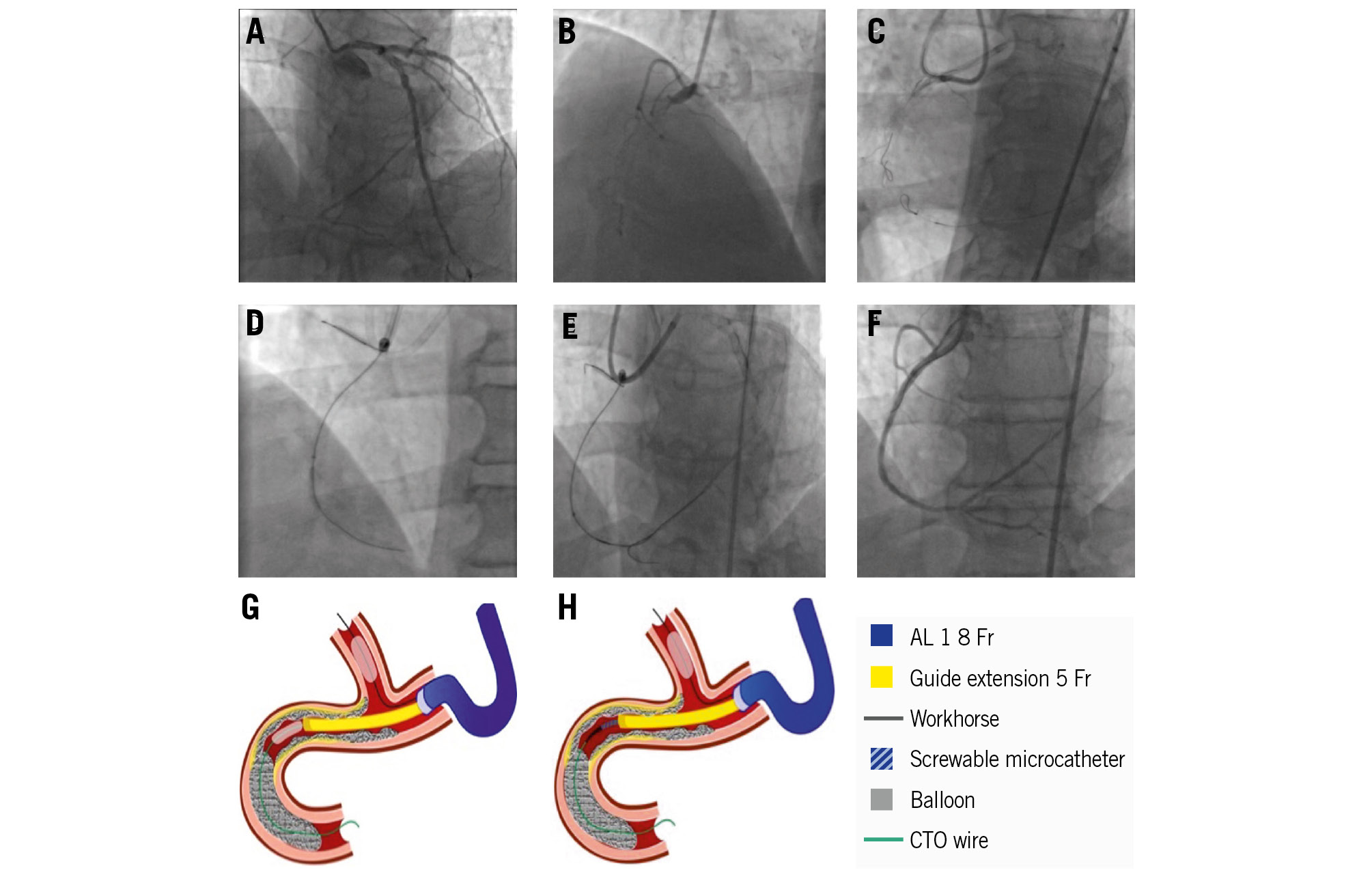
Figure 1. Anchor the Mother to Advance the Child (AMAC). A,B) Coronary angiography: right coronary CTO: blunt stamp, severe calcification, and extreme length involving the artery from the proximal part to the crux. The only interventional collateral option was an epicardial approach originating from the circumflex through the stent struts. C) Anterograde uncrossability, retrograde impenetrability, and failure of the subintimal tracking crossing. D-G) AMAC technique: while keeping an anchor balloon in the side branch, a guide extension catheter is advanced anterogradely within the same guide catheter adjacent to the balloon using the inchworming technique. E-H) Modified Anchor-Tornus technique: while keeping the anchor balloon and guide extension in place, a screwable microcatheter is advanced. F) The final result in a “leaving nothing behind” approach. AL: Amplatz Left; CTO: chronic total occlusion; Fr: French
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Diagnostic coronary angiography.
Moving image 2. Anchor the Mother to Advance the Child (AMAC) technique.
Moving image 3. Modified Anchor-Tornus technique.
Moving image 4. Final result.