Cory:
Unlock Your AI Assistant Now!
A 36-year-old man underwent percutaneous coronary intervention (PCI) of his right coronary artery (RCA) chronic total occlusion (CTO) due to refractory angina.
Dual angiography was performed using a 7 Fr Extra backup (EBU) 3.75 guide catheter in the left main and an 8 Fr Amplatz left (AL) 1 guide in the RCA (Figure 1A-Figure 1B, Moving image 1). The distal cap was accessed through septal collaterals using retrograde techniques (Figure 1C). The knuckle wire technique was employed to enter the extraplaque space of the CTO body using a polymer-jacketed wire.
The proximal CTO cap was engaged antegradely using a penetrative wire and microcatheter. This wire was exchanged for a polymer-jacketed wire, which was knuckled into the extraplaque space.
Reverse controlled antegrade and retrograde tracking (rCART) was then performed. The antegrade extraplaque space was predilated using a 3.0x15 mm balloon. An attempt to connect the retrograde Gladius Mongo (Asahi Intecc) wire with an antegrade 6 Fr LiquID guide extension (Seigla Medical) was unsuccessful. Subsequently, a 3.0x20 mm Ringer perfusion balloon catheter (RPBC; Teleflex), selected based on angiographic sizing of the vessel, was advanced over the antegrade wire and inflated to 8 atmospheres (Figure 1D, Moving image 2). rCART was performed by advancing the retrograde Gladius Mongo and Corsair Pro XS microcatheter (Asahi Intecc) into the central lumen of the RPBC and guide extension (Figure 1E, Moving image 3). Wire externalisation was then performed using a 350 cm externalisation wire. Intravascular ultrasound was used to size the RCA, which was predilated and treated using 2 overlapping stents, achieving a good result (Figure 1F, Moving image 4). The patient was discharged the same day.
The main challenge of rCART is advancing the antegrade and retrograde guidewires into a common space. The RPBC (Figure 1G) was recently introduced in the US for emergency use during large-vessel perforations1. Here, we describe an alternative use for this device. Figure 1H-Figure 1I show RPBC-facilitated rCART. The inflated RPBC enlarges the antegrade target by compressing the surrounding tissue, facilitating redirection of the retrograde wire into its central lumen. This approach appears advantageous compared to the use of a guide extension, as the retrograde wire often slides outside of the latter. However, it is important to note that guide extensions also provide the benefit of facilitating equipment delivery during the procedure. Additionally, utilising a 3.5 mm RPBC, which has an internal diameter of 0.079”, provides a larger wiring target compared to the maximum diameter of 0.072” that is currently possible with any available 8 Fr guide extension. These combined features may potentially improve the efficiency and success rate of retrograde CTO PCI. However, given the current high cost of the device, its use should be considered primarily for challenging cases in which conventional approaches have proven unsuccessful. Furthermore, additional experience is needed to fully assess its value compared to conventional guide extension-facilitated rCART.
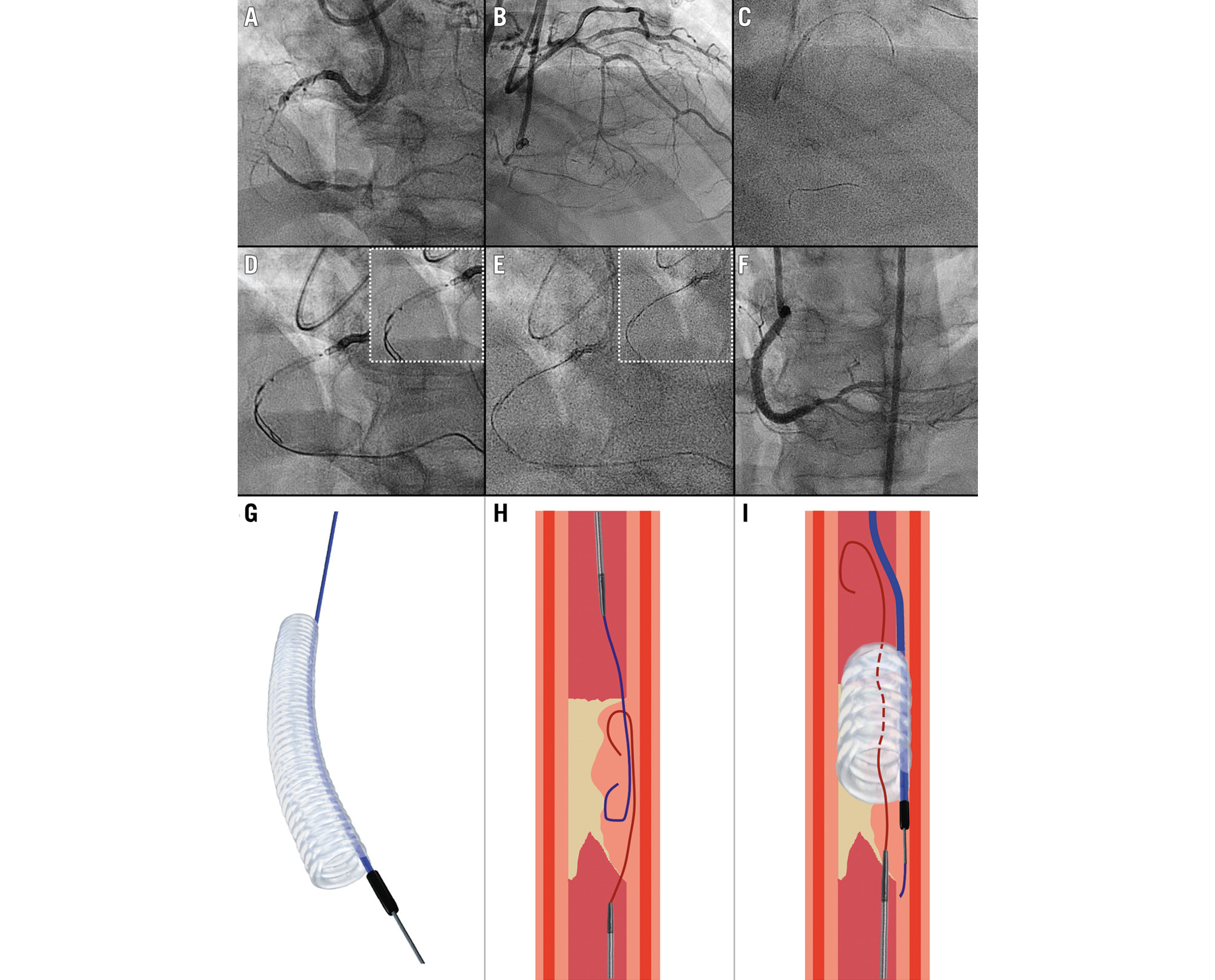
Figure 1. Reverse CART facilitated by the Ringer perfusion balloon catheter (RPBC). A) Mid-RCA CTO with (B) septal collaterals from the LAD. C) Septal surfing. D) Inflated RPBC (Teleflex). E) The retrograde wire enters the antegrade RPBC and guide catheter. F) Final angiographic result. G) The RPBC is a hollow balloon that allows interventional gear to be advanced through it when inflated. H) Antegrade and retrograde knuckle wires in the occlusion. I) RPBC-facilitated rCART: the retrograde wire enters the antegrade space that is dilated and kept open by the inflated RPBC. CTO: chronic total occlusion; LAD: left anterior descending artery; RCA: right coronary artery; rCART: reverse controlled antegrade and retrograde tracking
Conflict of interest statement
W.L. Lombardi received consulting fees from Asahi Intecc, Abiomed, Boston Scientific, Medtronic, Siemens, and Teleflex; receives royalties from Asahi Intecc; owns equity in Reflow Medical; and his spouse is a Reflow Medical employee. L. Azzalini received consulting fees from Teleflex, Abiomed, GE HealthCare, Reflow Medical, Shockwave, Abbott, and Cardiovascular Systems Inc; received a research grant from Abiomed; serves on the advisory boards of Abiomed and GE HealthCare; and owns equity in Reflow Medical. P. Ng has no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Baseline angiogram of the RCA CTO.
Moving image 2. Inflated Ringer balloon.
Moving image 3. The retrograde wire engages the inflated Ringer balloon, the guide extension, and the antegrade guide.
Moving image 4. Final result.