Cory:
Unlock Your AI Assistant Now!
A 77-year-old female with idiopathic pulmonary fibrosis and coronary artery disease presented with severe symptomatic heart failure (New York Heart Association Class IV). Echocardiography revealed severe mitral annular calcification (MAC) with reduced leaflet mobility, resulting in severe mitral stenosis (mean gradient 12 mmHg, peak gradient 23 mmHg) and mild mitral regurgitation (MR). Additional findings included moderate tricuspid regurgitation, severe pulmonary hypertension (systolic pulmonary arterial pressure of 80 mmHg), and a left ventricular ejection fraction of 45%. Cardiac computed tomography (CT) confirmed severe circumferential MAC (MAC score=9) and a porcelain aorta. Due to prohibitive surgical risk, the Heart Team opted for transfemoral transcatheter mitral valve replacement (TMVR).
The preprocedural planning CT (Figure 1A) predicted a neo-left ventricular outflow tract (neo-LVOT) area of 80 mm² for a 29 mm MyVal prosthesis (Meril Life Sciences). The anterior mitral leaflet (AML) measured 28 mm, and the interventricular septal thickness was 11 mm. These findings raised concerns about potential LVOT obstruction due to the long AML, prompting the decision to use the balloon-assisted translocation of the mitral anterior leaflet (BATMAN) technique, a within-leaflet transcatheter heart valve implantation strategy.
Following inferior and posterior transseptal puncture, a steerable guide catheter was advanced into the left atrium. Through a multipurpose catheter, we used the back end of a 0.035” wire and electrified it to perforate the AML at the mid-A2 segment, approximately 5-7 mm from its base, avoiding a calcific nodule and the aortomitral curtain (Figure 1B, Moving image 1). After exchanging for two SAFARI² wires (Boston Scientific), a 14 mm Atlas balloon (BD) was used for the AML dilation (Figure 1C, Moving image 1). After that, acute MR was observed (Moving image 1), so the balloon was immediately pulled back, a septostomy was carried out and the balloon was advanced into the leaflet once again; this eliminated the MR.
Simultaneously, using the balloon and one wire as a buddy balloon and buddy wire, a 29 mm MyVal prosthesis was loaded on the second wire and positioned across the AML. After removing the balloon and the first wire, the valve was inflated under rapid pacing (Figure 1D). Post-deployment, the valve achieved optimal haemodynamic performance with no mitral gradient and no systolic gradient across the LVOT, showing no paravalvular leakage (Moving image 1). Despite minor protrusion of the valve’s ventricular open cells into the LVOT, no obstruction occurred due to the absence of the AML (Figure 1E, Figure 1F, Moving image 1).
This case demonstrates the feasibility of transfemoral TMVR using the BATMAN technique for severe MAC and a long AML. Previous reports have described the use of this technique mainly in valve-in-ring1, but also in valve-in-MAC23 implantation. By perforating and displacing the AML, this technique mitigates LVOT obstruction while providing prosthesis stability and sealing. The BATMAN technique involves mechanical tearing of the AML, which introduces several theoretical risks. Unlike the controlled linear electrosurgical laceration used in techniques like laceration of the anterior mitral leaflet to prevent outflow obstruction (LAMPOON), mechanical tearing is less predictable, raising concerns about non-central tearing. This could lead to tissue prolapse, inadequate sealing, or disruption of critical structures such as the aortomitral curtain.
We chose not to use an intra-aortic balloon pump, often recommended in LAMPOON, as haemodynamic stability was maintained throughout the procedure.
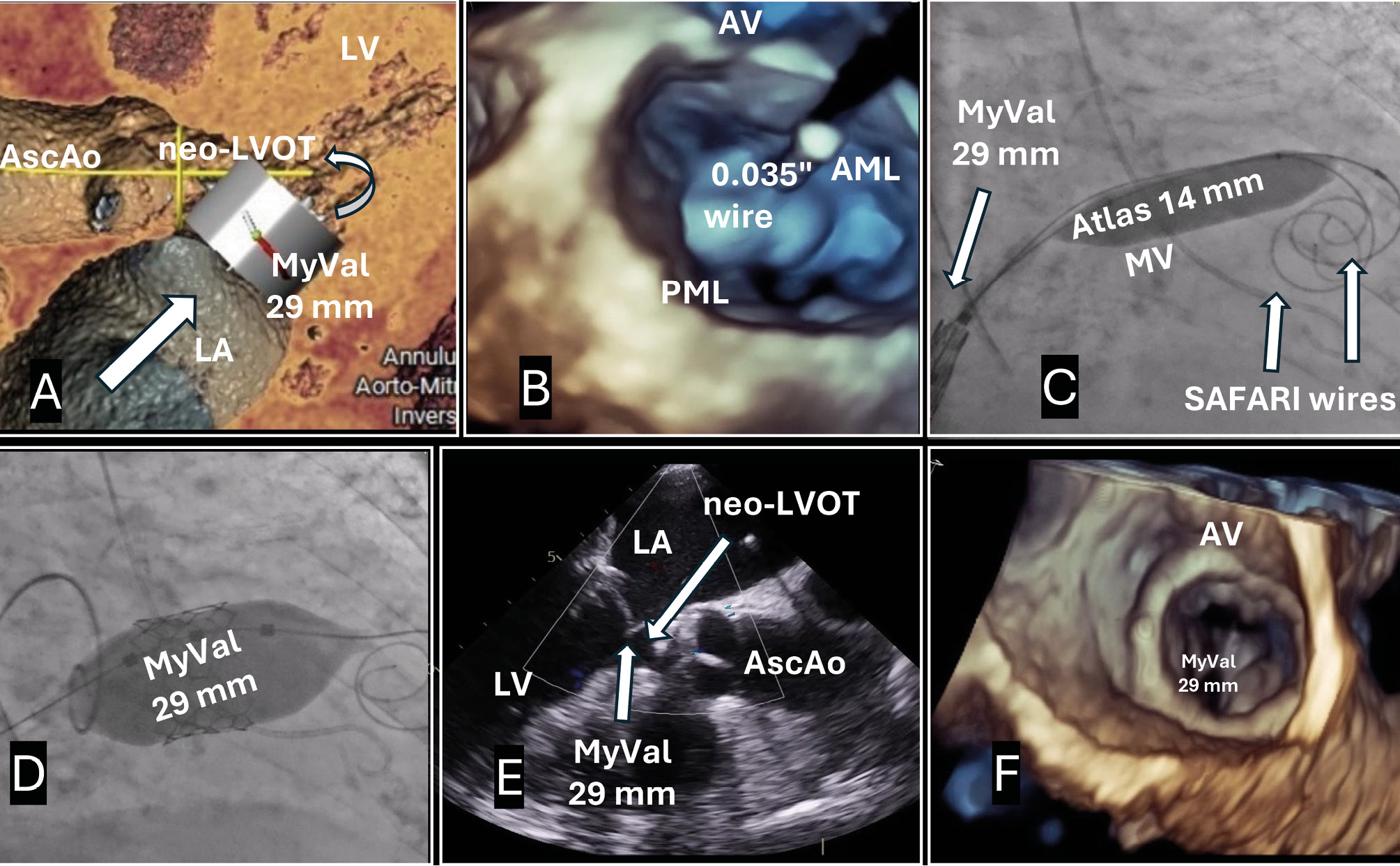
Figure 1. Balloon-assisted translocation of the anterior mitral leaflet to facilitate native mitral replacement. A) Preprocedural CT showing severe MAC and predicted neo-LVOT area. B) AML perforation site. C) Side-by-side predilatation balloon and valve delivery systems. D) Valve inflation under rapid pacing. E,F) Final result. Atlas by BD; MyVal by Meril Life Sciences; SAFARI² by Boston Scientific. AML: anterior mitral leaflet; AscAo: ascending aorta; AV: aortic valve; LA: left atrium; LV: left ventricle; LVOT: left ventricular outflow tract; MAC: mitral annular calcification; MV: mitral valve; PML: posterior mitral leaflet
Conflict of interest statement
The authors have no conflicts of interest related to this manuscript to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Procedural steps.