Cory:
Unlock Your AI Assistant Now!
Immersed in our everyday activities and busy work schedules, we run the risk of failing to appreciate our privileged position as interventional cardiologists to witness and gain insights into many aspects of cardiac physiology. Fortunately, every now and then, we come across fresh observations that support or reinforce a body of knowledge largely obtained in the experimental laboratory. This is indeed the case for the research published on coronary flow regulation in this issue of EuroIntervention by Marin and colleagues1.
To trace the context of this research, we should go back to the French physiologist Claude Bernard, who, in 1865, coined the term “milieu intérieur” and the associated concept of homeostasis to describe the steady internal physical and chemical conditions that are autonomously maintained in living organisms. One specific case of homeostasis is regulating arterial blood supply under shifting conditions. In 1902, Bayliss found that hindlimb arterioles regulate flow through an intrinsic myogenic reflex that reacts to variations of intraluminal pressure, thus keeping flow constant before arterial pressure shifts2, and in 1959, Lassen demonstrated the existence of a cerebral autoregulation curve maintaining stable blood flow across a wide arterial pressure range3. In the coronary circulation, Gould and colleagues demonstrated that, when a coronary stenosis is present, autoregulation causes compensatory microcirculatory dilatation to preserve resting blood supply to the myocardium4. The mechanism proved to be so effective that only when the severity of the stenosis reaches 85% diameter stenosis or more, this autoregulatory reserve became exhausted, and resting flow declined. This finding explains why myocardial ischaemia does not occur in the resting state until the stenosis becomes critical. Effort angina, on the other hand, is explained by the fact that maximal hyperaemic flow decreases gradually as stenosis severity progresses.
In 2015, the European IDEAL collaborative study reproduced the findings of Gould et al for the first time in 301 patients using intracoronary Doppler flow wires5. The study revealed the progressive increase of the transstenotic pressure gradient with increasing stenosis severity and the compensatory reduction of microvascular resistance to maintain a constant resting hyperaemic flow, as Figure 1 shows. Now, Marin et al report the findings of an elegant study in 52 patients based on continuous saline thermodilution measurements, a technique which provides highly accurate measurements of coronary blood flow and microvascular resistance1, confirming that percutaneous coronary intervention (PCI) reduces both resting and hyperaemic epicardial resistance. Under resting conditions, relieving the stenosis means that the microcirculation constricts once again, to avoid unnecessarily oversupplying the myocardium of precious oxygen-rich arterial blood. On the contrary, when microvascular constriction in the smaller coronary arterioles is abolished by high-dose adenosine, microcirculatory resistance remains unchanged after PCI. Because the stenotic epicardial resistor is removed, hyperaemic coronary flow increases after PCI, and the authors find that fractional flow reserve (FFR) predicts this increase in hyperaemic flow. These changes in coronary haemodynamics can also be worked out from Figure 1 as a leftward shift related to decreasing stenosis severity with PCI.
The findings of the authors are of great interest, not only to confirm the experimental observations made previously, but also to address any remaining scientific doubt pertaining to the validity of physiological frameworks of both coronary autoregulation and FFR as the present observations were made (1) within humans, (2) under the most controlled circumstances by measuring within the same patient in the presence of a stenosis (pre-PCI) and without a stenosis (post-PCI), (3) using an advanced method to accurately measure coronary blood flow, and (4) confirming the observations not just in a single patient, but in a sufficiently large cohort. For all this, and for reminding us of the importance of keeping our curiosity alive as clinicians and scientists, the authors deserve heartfelt congratulations.
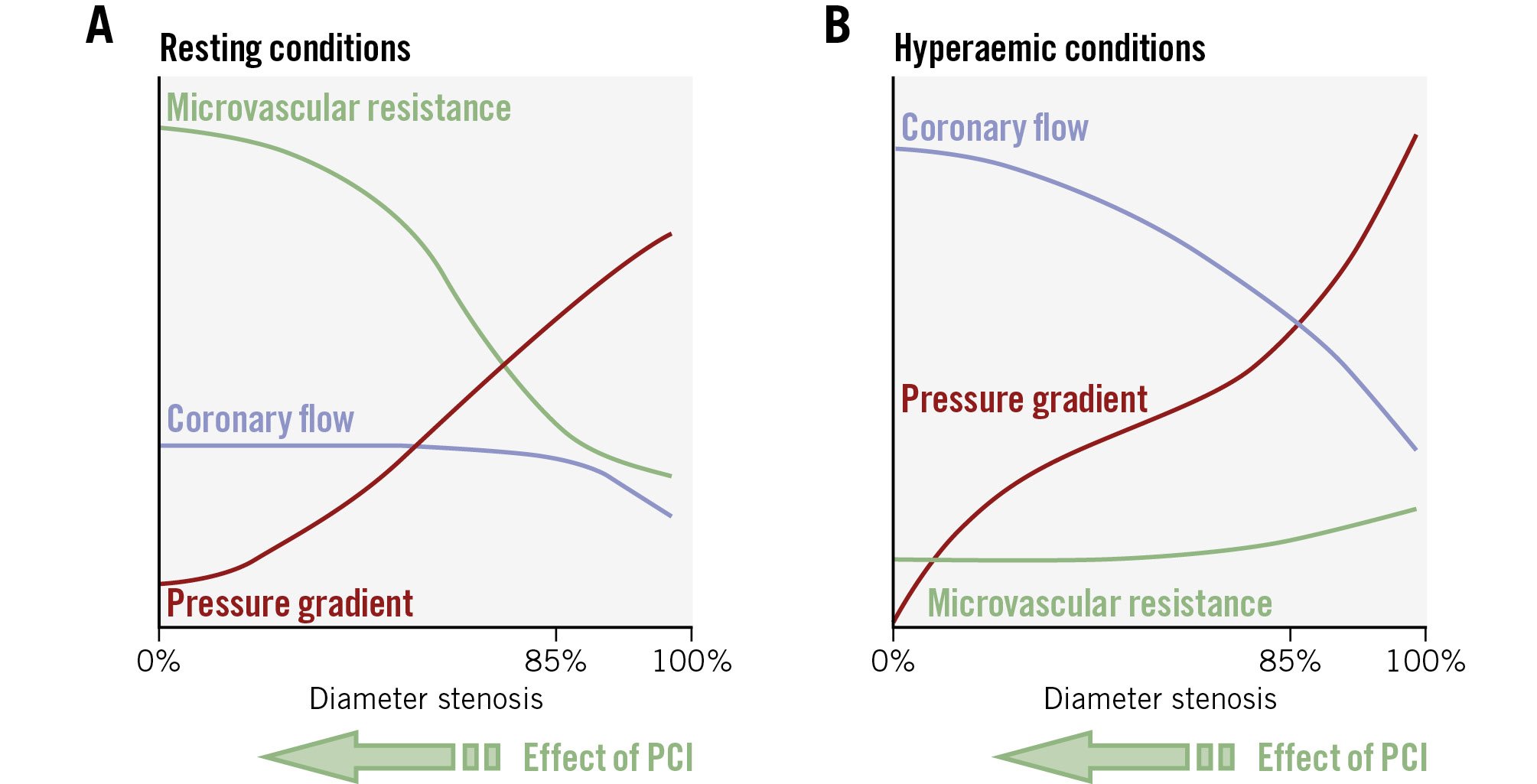
Figure 1. The relationships between the transstenotic pressure gradient, stenosis severity, microvascular resistance, and coronary flow. The graphs demonstrate these relationships at rest (A) and during hyperaemia (B). PCI: percutaneous coronary intervention
Conflict of interest statement
J. Escaned declares consulting fees and honoraria from Abbott, Boston Scientific, and Philips. G. de Waard has no conflicts of interest to declare.