Suture-based vascular closure device (VCD) strategies were the only available percutaneous option for large-bore arterial access site closure for more than two decades. A continuously increasing demand for more ideal solutions, particularly driven by the growing number of transfemoral transcatheter aortic valve implantation (TAVI) procedures, has prompted the development of novel, tailored large-bore VCDs. In 2016, the large-bore plug-based MANTA device (Teleflex) was introduced, raising hopes for faster and more secure vascular closure, as suggested by early non-randomised studies123. However, the MANTA device failed to meet these high expectations in two randomised controlled trials (RCTs). While the small-sized MASH trial demonstrated no superiority using two Perclose ProGlide devices (Abbott) compared to a suture-based strategy4, the larger CHOICE-CLOSURE trial reported significantly higher vascular complication rates with the MANTA plug5. Despite these disappointing results from two RCTs, the comparison of suture-based and plug-based VCDs remains contentious.
In this issue of EuroIntervention, Grundmann et al provide a large propensity score-matched registry analysis (the Plug or sUture based vascuLar cloSurE after TAVI [PULSE] registry), further tipping the scale in favour of suture-based techniques6. Out of 10,120 patients who underwent transfemoral TAVI between 2016 and 2021 at 10 German centres, 900 MANTA patients and 1,800 ProGlide patients were matched and analysed according to the most recent Valve Academic Research Consortium-3 criteria7. The primary endpoint of access site-related vascular complications was observed in 14.9% of the MANTA patients and 10.3% of the ProGlide patients (p<0.001). Consistent with the previously mentioned RCTs, this was primarily driven by a two-times higher minor vascular complication rate (11.3% vs 5.8%; p<0.001) in MANTA patients. Notably, bleeding rates were higher and the need for additional interventions like endovascular ballooning or stenting was more common in the MANTA group.
The authors should be praised for reporting outcomes from a large registry-based analysis comparing both closure device strategies and for using contemporary, highly sensitive outcome definitions. And while their findings are in contrast with previous smaller observational studies that included selected patient populations, they reinforce the superiority of suture-based techniques that was previously seen in RCTs (Figure 1). The greatest weakness of the MANTA-based technique lies in the fact that vessel access is lost after deployment of the collagen plug, making further direct escalation via the primary access route practically impossible. This major limitation renders the use of MANTA an “all or nothing” approach, with an obligatory binary outcome (success or failure). And importantly, failure of the MANTA technique can seldom be corrected without additional endovascular or surgical interventions. On the contrary, the suture-based approach allows for the additional use of similar or alternative closure devices to optimise haemostasis and appears, in general, to be more “forgiving”. In addition, bleeding due to suboptimal vascular closure remains common after use of the MANTA device, though the lack of difference in the incidence of pseudoaneurysms in this registry probably reflects the absence of systematic granular assessment in the setting of a retrospective study.
Of note, the analysis by Grundmann et al includes various ProGlide-based strategies. While 67.6% of patients underwent the classic double ProGlide technique, 9.6% received a single ProGlide, and 22.8% were treated with a combination of one ProGlide and one small plug (Angio-Seal [Terumo]). The latter “hybrid” approach has become increasingly popular in recent years, and the recently published randomised ACCESS-TAVI trial has reported superior outcomes compared to the classic double ProGlide strategy8. Importantly, although now widely used, ultrasound-guided access was performed in only 1.9% of patients in the PULSE registry. Consequently, the impact of ultrasound guidance (for both access and closure) on the relative efficacy of both strategies cannot be extrapolated from this study.
Does this mean large-bore plug-based VCDs should be abandoned? In recent years, different variations of puncture and closure techniques have been developed and their practicality has been demonstrated in various studies. As of today, an ultrasound-guided puncture and a hybrid VCD approach (primary suture-based complemented with a small plug) seem to provide the highest possible safety and efficacy. The use of the larger MANTA plug should probably be reserved for potential bailout indications if suture-based closure fails to achieve adequate haemostasis9. In this context, simple, step-wise escalation algorithms, such as the one recently described from the TAVI-MultiCLOSE registry, may provide a pragmatic, reproducible approach for large-bore vascular closure10. And while further refinements in technique and technology of non-suture-based approaches should still be encouraged, they would first need to prove themselves against an old unbeaten champion.
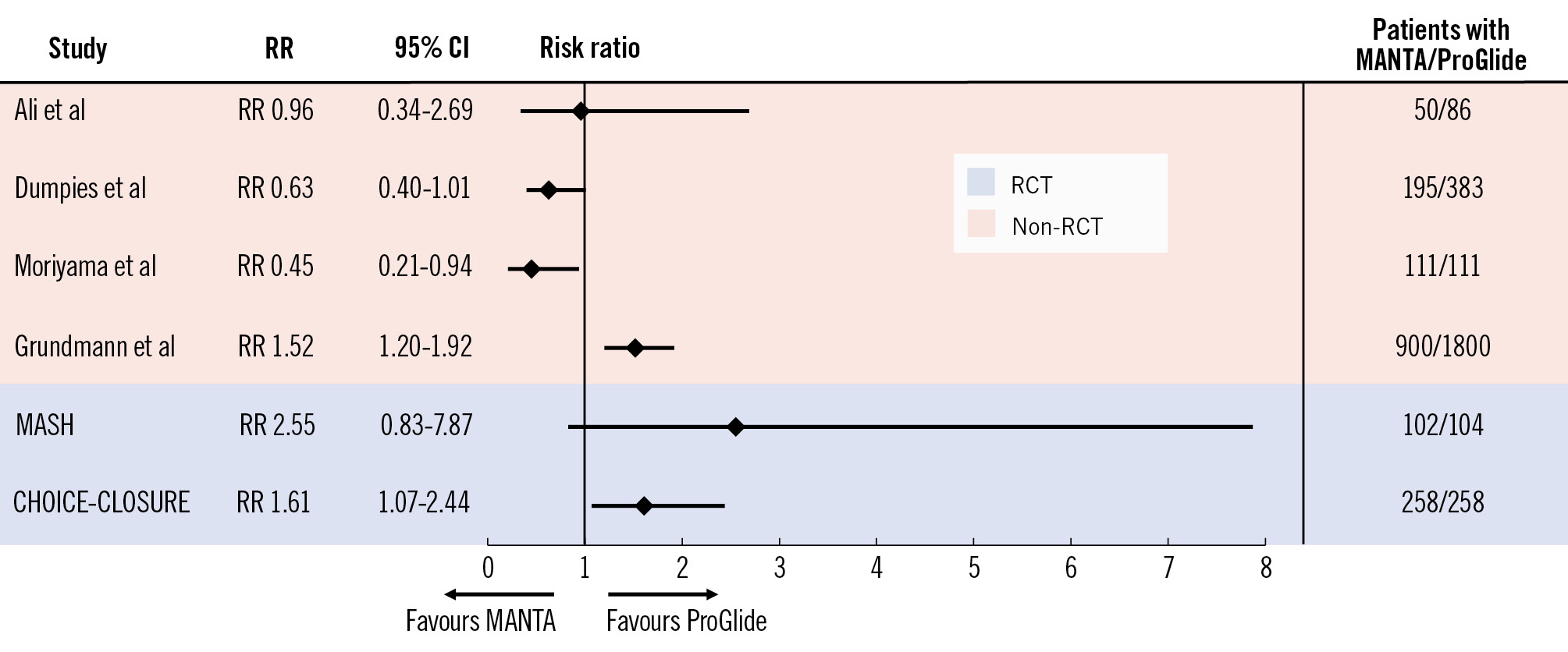
Figure 1. Main access site-related vascular complications with MANTA- versus ProGlide-based arterial access site closure across various observational and randomised clinical studies. CI: confidence interval; RCT: randomised controlled trial; RR: risk ratio
Conflict of interest statement
M. Abdel-Wahab reports that his hospital receives speaker honoraria and/or consultancy fees on his behalf from Boston Scientific, Medtronic, and Edwards Lifesciences. O. Dumpies has no conflicts of interest to declare.
