Cory:
Unlock Your AI Assistant Now!
Abstract
BACKGROUND: Acute coronary syndrome (ACS) is frequently accompanied by newly diagnosed atrial fibrillation (AF).
AIMS: We aimed to compare the risk of major adverse cardiovascular events (MACE) in ACS patients presenting with known, newly diagnosed, or no AF.
METHODS: In our multicentre, prospective registry study, we included patients with confirmed ACS. Patients are classified as having known, newly diagnosed or no AF. Newly diagnosed AF is subdivided according to the duration of the episode, time of onset, post-coronary artery bypass graft (CABG) or spontaneous occurrence, and treatment with oral anticoagulants (OAC). The primary endpoint is MACE at 1 year. Key secondary endpoints include ischaemic stroke and bleeding complications.
RESULTS: Amongst 4,433 patients with confirmed ACS, 3,598 (81.2%) had no AF, 438 (9.9%) had newly diagnosed AF, and 397 (9.0%) had known AF. The rates of OAC treatment at discharge were 53.4% in patients with newly diagnosed AF and 89.2% in patients with known AF. After adjusting for baseline imbalances, only new AF was independently associated with increased rates of MACE, whereas known AF was not (hazard ratio [HR] 1.52, 95% confidence interval [CI]: 1.19-1.90 and HR 0.93, 95% CI: 0.70-1.23). For ACS patients with newly diagnosed AF, episodes lasting >24 hours were associated with a higher risk of MACE compared to episodes <24 hours (HR 1.99, 95% CI: 1.36-2.93). Episodes of new AF occurring post-CABG had more favourable outcomes compared to spontaneously occurring new AF (HR for MACE 0.52, 95% CI: 0.31-0.86). OAC treatment rates were higher in the new AF subcategories with higher rates of MACE and ischaemic stroke.
CONCLUSIONS: Newly diagnosed AF in ACS patients was associated with higher rates of MACE and ischaemic stroke compared to ACS patients without or with known AF. Among the ACS patients with new AF, an episode lasting >24 hours was associated with worse outcomes than shorter episodes, while post-CABG occurrence of AF showed relatively better outcomes compared to spontaneously occurring AF. Only 53% of new AF patients were discharged on OAC therapy versus 89% with known AF.
Atrial fibrillation (AF) is a commonly coexisting condition in patients that present with acute coronary syndrome (ACS). Both conditions share multiple risk factors, such as older age, obesity, hypertension, and diabetes mellitus. As a result, around 10% of patients with a recent percutaneous coronary intervention (PCI) have AF, and 25-35% of patients with AF have coronary artery disease1. A history of AF in patients with ACS was independently associated with worse outcomes in several observational studies23.
Concomitant treatment of AF and ACS is complicated. Treatment of AF, based on the CHA2DS2-VASc score, consists, amongst others, of oral anticoagulants (OAC) to lower the risk of ischaemic stroke4. Antithrombotic treatment after ACS, on the other hand, consists of dual antiplatelet therapy (DAPT) to prevent recurrent myocardial infarction (MI)5. The combination of OAC and DAPT, called triple therapy, is accompanied by high rates of bleeding complications. Therefore, current guidelines recommend a combined treatment of OAC with a P2Y12 inhibitor, with only a short course of aspirin early after the ACS for most patients with concomitant AF and ACS56.
While the need for antithrombotic treatment in patients with known AF stands without doubt, less is known about the prognosis and optimal antithrombotic treatment of newly diagnosed AF during an ACS. It is unclear whether new AF during an ACS event confers a similar increased risk for ischaemic stroke as AF that was already known of before the ACS and whether it should be treated similarly. Observational studies show that patients who suffer from concomitant AF and ACS receive potentially inadequate antithrombotic treatment, as OAC is not always prescribed, especially not in newly diagnosed AF7. Therefore, it is of great importance whether newly diagnosed AF in ACS patients confers a higher risk of thromboembolic events.
In this cohort study, we aim to elucidate the incidence and characteristics of new AF in patients presenting with ACS. Clinical outcomes are compared between patients without, with new, or with known AF. Furthermore, episode characteristics and the antithrombotic treatment of new AF are evaluated, and their associations with major adverse cardiovascular events (MACE), and especially ischaemic stroke, are explored.
Methods
STUDY DESIGN AND POPULATION
This study was executed within the FORCE-ACS registry. The design of this registry has been published previously8. Briefly, the FORCE-ACS registry is an ongoing, multicentre, prospective registry which includes ACS patients from 9 interventional and non-interventional cardiac centres located in different regions of the Netherlands.
For this analysis, only patients with at least 1 year of complete follow-up were selected. We included hospitalised adult patients with a confirmed diagnosis of ST-segment elevation myocardial infarction (STEMI), non-ST-segment elevation myocardial infarction (NSTEMI), unstable angina pectoris (UAP) or semirecent MI (MI with significant ST-segment deviations and significantly elevated cardiac enzymes presenting out of the window period for primary PCI, i.e., typically 12 hours to 5 days after symptom onset). Patients were excluded if they had incomplete 1-year follow-up or were discharged with a diagnosis of type 2 ACS, Takotsubo syndrome, non-specified chest pain, or a non-cardiac or other cardiac diagnosis.
DATA COLLECTION
The FORCE-ACS registry comprised information on medical history, the index ACS admission, (antithrombotic) treatment, and ischaemic and bleeding outcomes during follow-up. For the purpose of this study, data including outcome events from hospital admission to 1 year after discharge were used.
Additional data on the occurrence of AF during hospitalisation was retrospectively collected. All electrocardiograms (ECGs) during hospitalisation (including ambulance ECGs if available) and discharge letters were assessed for episodes of AF. Based on medical history and ECGs, patients were classified as (1) patients without AF, (2) patients with new AF, or (3) patients with known AF. Additionally, episodes of new AF were classified based on the time of onset (early: i.e., within the first 24 hours of presentation, or late: i.e., after 24 hours of presentation), the duration (short: i.e., <24 hours or long: i.e., >24 hours) and if the patient had undergone coronary artery bypass graft (CABG) during admission, whether or not the episode occurred in the post-CABG setting. Patients with multiple short paroxysms of AF occurring within a timespan of over 24 hours, were classified as having an AF duration of >24 h. Both atrial fibrillation and atrial flutter were classified as episodes of AF. Furthermore, antithrombotic treatment was evaluated.
OUTCOMES
The primary outcome was MACE, a composite of all-cause mortality, MI, and ischaemic stroke. Secondary outcomes included ischaemic stroke and bleeding complications.
Mortality was defined according to the Academic Research Consortium (ARC)-2 criteria9, MI according to the 4th Universal Definition of MI10, ischaemic stroke according to the Valve Academic Research Consortium (VARC) criteria11, and bleeding according to the Bleeding Academic Research Consortium (BARC) criteria12. Major bleeding was defined as BARC type 3 or 5. A clinical endpoint committee adjudicated all clinical endpoints8.
All events from admission to 1-year follow-up were included in the analyses, including periprocedural events. As in-hospital antithrombotic treatment was not captured in the database, the sequential order of, e.g., OAC use and in-hospital events could not be determined. Therefore, the analyses stratified for OAC use only analysed events post-discharge.
STATISTICAL ANALYSIS
Baseline characteristics are presented as numbers and percentages for categorical variables, and were compared by the chi-square test. Continuous variables are reported as mean and standard deviation (SD) and were compared by analysis of variance (ANOVA).
Clinical outcomes were visualised by Kaplan-Meier curves. The outcomes of MACE and all-cause mortality were examined using unadjusted and multivariable adjusted Cox proportional hazard analyses. The log-rank test was used to test for differences between groups. The outcomes of stroke, myocardial infarction and bleeding were examined using unadjusted and multivariable-adjusted Fine-Gray subdistribution hazard models to account for the competing risk of death. To avoid bias due to complete case analyses, multiple imputation using the mice package was performed.
To adjust for potential confounders, we considered the following variables of clinical interest for MACE: age (as a continuous variable), sex, smoking status, hypertension, baseline estimated glomerular filtration rate (eGFR; as a continuous variable), prior stroke, peripheral artery disease, prior revascularisation (PCI or CABG), prior heart failure, prior MI (STEMI or NSTEMI), CHA2DS2-VASc score, discharge diagnosis (STEMI, NSTEMI, UAP, or semirecent MI), Killip class, and out-of-hospital cardiac arrest (OHCA) at presentation. For bleeding events, we considered the following variables of clinical interest: age (as a continuous variable), sex, baseline haemoglobin (as a continuous variable), baseline platelet count (as a continuous variable), baseline eGFR (as a continuous variable), prior stroke, and prior bleeding leading to hospitalisation.
A p-value≤0.05 was considered statistically significant. All statistical analyses were performed using R, version 4.3.1 (R Foundation for Statistical Computing).
Results
STUDY POPULATION
A total of 4,433 patients with a confirmed diagnosis of ACS were included between 2014 and 2021 (Figure 1). Of these patients, 3,598 (81.2%) were without AF, 438 (9.9%) were newly diagnosed with AF during hospitalisation, and 397 (9.0%) had known AF. Of the patients with new AF, 215 (53.5%) were discharged with OAC, and of the patients with known AF, 340 (89.2%) were discharged with OAC.
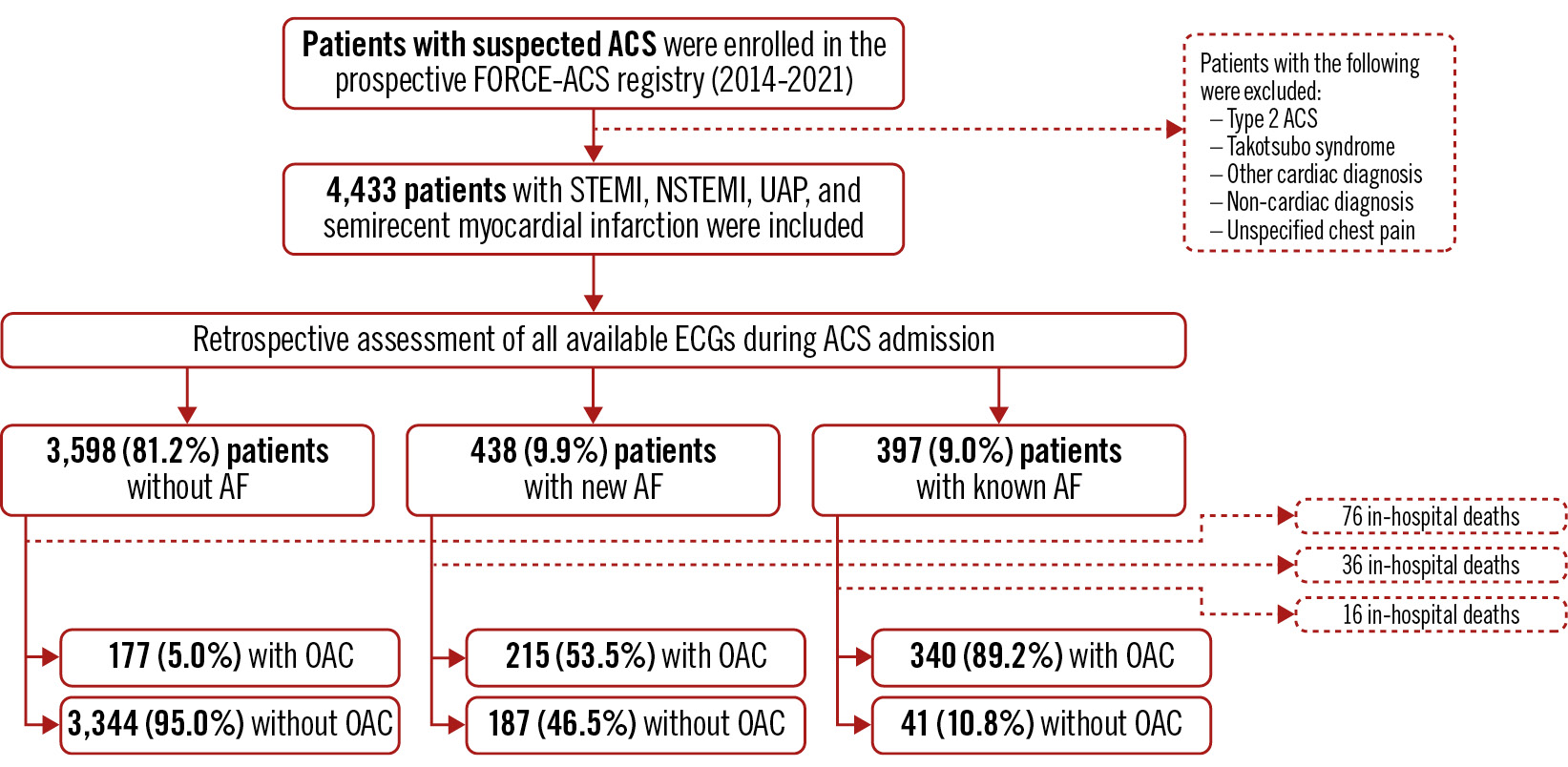
Figure 1. Inclusion flowchart. ACS: acute coronary syndrome; AF: atrial fibrillation; ECG: electrocardiogram; NSTEMI: non-ST-segment elevation myocardial infarction; OAC: oral anticoagulants; STEMI: ST-segment elevation myocardial infarction; UAP: unstable angina pectoris
BASELINE CHARACTERISTICS OF PATIENTS WITH NO, NEW, OR KNOWN ATRIAL FIBRILLATION
The baseline characteristics of the included patients according to AF status are shown in Table 1. As compared to patients without AF, patients with new AF and known AF were older (mean age 65, 71, and 74 years, respectively; p<0.001) and had significantly more comorbidities. A medical history of hypertension, diabetes mellitus, stroke, peripheral artery disease, congestive heart failure, and clinically relevant bleeding gradually increased from patients without, to patients with new and known AF (p<0.01 for all). A history of MI, PCI, and/or CABG was more prevalent in patients with known AF as compared to those with no or new AF. Sex and body mass index did not differ between the groups.
Upon presentation, patients with new AF were more likely to present with Killip class III or IV, or OHCA, compared to patients with no or known AF (p<0.001). Presentation with a semirecent MI was more common amongst patients with new AF, whilst patients with known AF were less likely to present with STEMI and more likely to present with NSTEMI or UAP (p<0.001). Infarct size, represented by the maximum creatine kinase (CK) values, was largest in new AF patients, and accordingly, left ventricular ejection fraction (LVEF) at discharge was worst in new AF patients (p<0.001 for both). Patients with new AF were more likely to have been treated with CABG during hospitalisation than patients without or with known AF (33.1%, 9.6%, and 11.6%; p<0.001).
Table 1. Clinical characteristics of ACS patients according to AF status.
| No AF n=3,598 | New AF n=438 | Known AF n=397 | p-value | % missing | |
|---|---|---|---|---|---|
| Demographics and cardiovascular risk factors | |||||
| Age, years | 65±12 | 71±11 | 74±9 | <0.001 | 0.0 |
| Female sex | 1,020 (28.3) | 108 (24.7) | 117 (29.5) | 0.22 | 0.0 |
| Body mass index, kg/m² | 27.4±4.4 | 27.3±4.2 | 27.0±4.3 | 0.30 | 6.0 |
| Hypertension | 1,926 (54.5) | 270 (62.1) | 283 (73.3) | <0.001 | 1.7 |
| Hypercholesterolaemia | 1,992 (57.4) | 250 (59.2) | 225 (59.8) | 0.55 | 3.7 |
| Diabetes mellitus | 727 (20.4) | 108 (24.8) | 110 (28.1) | <0.001 | 0.9 |
| Active smoker | 1,118 (31.9) | 103 (24.1) | 57 (15.0) | <0.001 | 2.6 |
| Medical history | |||||
| Myocardial infarction | 715 (19.9) | 81 (18.5) | 142 (36.2) | <0.001 | 0.3 |
| PCI | 749 (20.9) | 70 (16.0) | 140 (35.5) | <0.001 | 0.2 |
| CABG | 273 (7.6) | 31 (7.1) | 101 (25.4) | <0.001 | 0.0 |
| Stroke | 276 (7.7) | 58 (13.2) | 70 (17.6) | <0.001 | 0.0 |
| Peripheral artery disease | 258 (7.2) | 51 (11.6) | 69 (17.4) | <0.001 | 0.0 |
| Congestive heart failure | 89 (2.5) | 20 (4.6) | 52 (13.1) | <0.001 | 0.0 |
| Clinically relevant bleeding | 124 (3.5) | 29 (6.7) | 48 (12.3) | <0.001 | 1.2 |
| Laboratory results | |||||
| Haemoglobin, mmol/L | 8.6±1.0 | 8.5±1.1 | 8.3±1.1 | <0.001 | 1.0 |
| Platelet count, 109/L | 252±74 | 248±81 | 234±97 | <0.001 | 3.8 |
| eGFR, mL/min | 78±21 | 69±23 | 65±23 | <0.001 | 0.3 |
| ACS presentation | |||||
| Discharge diagnosis | <0.001 | 0.0 | |||
| UAP | 321 (8.9) | 22 (5.0) | 57 (14.4) | ||
| NSTEMI | 1,648 (45.8) | 186 (42.5) | 263 (66.2) | ||
| STEMI | 1,515 (42.1) | 197 (45.0) | 69 (17.4) | ||
| Semirecent infarction | 114 (3.2) | 33 (7.5) | 8 (2.0) | ||
| Killip class upon admission | <0.001 | 0.9 | |||
| I | 3,173 (89.0) | 341 (77.9) | 315 (80.4) | ||
| II | 336 (9.4) | 69 (15.8) | 68 (17.3) | ||
| III | 19 (0.5) | 9 (2.1) | 5 (1.3) | ||
| IV | 37 (1.0) | 19 (4.3) | 4 (1.0) | ||
| Out-of-hospital cardiac arrest | 134 (3.7) | 40 (9.1) | 13 (3.3) | <0.001 | 0.1 |
| Number of diseased coronary vessels | <0.001 | 6.2 | |||
| 0 | 231 (6.7) | 11 (2.8) | 24 (7.1) | ||
| 1 | 1,519 (44.3) | 116 (29.7) | 115 (33.9) | ||
| 2 | 956 (27.9) | 103 (26.3) | 91 (26.8) | ||
| 3 | 703 (20.5) | 159 (40.7) | 108 (31.9) | ||
| Graft dysfunction | 20 (0.6) | 2 (0.5) | 1 (0.3) | ||
| CK max, U/L | 871±1,745 | 1,555±3,208 | 517±973 | <0.001 | 10.9 |
| CABG during admission | 343 (9.6) | 145 (33.1) | 46 (11.6) | <0.001 | 0.2 |
| LVEF at discharge | <0.001 | 11.3 | |||
| >50% | 2,232 (71.3) | 235 (56.0) | 243 (63.8) | ||
| 30-50% | 765 (24.4) | 130 (31.0) | 104 (27.3) | ||
| <30% | 134 (4.3) | 55 (13.1) | 34 (8.9) | ||
| Antithrombotic medication at discharge | |||||
| Aspirin | 3,365 (93.5) | 252 (57.5) | 120 (30.2) | <0.001 | 0.0 |
| Clopidogrel | 811 (22.6) | 222 (50.8) | 297 (75.0) | <0.001 | 0.1 |
| Ticagrelor or prasugrel | 2,550 (71.0) | 147 (33.6) | 50 (12.6) | <0.001 | 0.1 |
| Oral anticoagulants | 177 (5.0) | 215 (53.5) | 340 (89.2) | <0.001 | 0.0 |
| Data are presented as mean±SD or n (%). P-values in bold indicate statistical significance. ACS: acute coronary syndrome; AF: atrial fibrillation; CABG: coronary artery bypass graft; CK: creatine kinase; eGFR: estimated glomerular filtration rate; LVEF: left ventricular ejection fraction; NSTEMI: non-ST-segment elevation myocardial infarction; PCI: percutaneous coronary intervention; SD: standard deviation; STEMI: ST-segment elevation myocardial infarction; UAP: unstable angina pectoris | |||||
CLINICAL OUTCOMES ACCORDING TO ATRIAL FIBRILLATION STATUS
Kaplan-Meier curves of MACE and ischaemic stroke according to AF status during 1 year of follow-up are shown in the Central illustration. The 1-year incidences of MACE in patients without, with new, or with known AF were 9.6%, 23.7%, and 16.6%, respectively. Ischaemic stroke occurred in 1.3%, 3.4%, and 1.0% of patients, respectively. All-cause mortality was 4.8%, 16.9%, and 10.1% at 1 year, respectively.
After adjusting for baseline imbalances, only new AF but not known AF was significantly associated with increased MACE (hazard ratio [HR] 1.52, 95% confidence interval [CI]: 1.19-1.90; p<0.001 and HR 0.93, 95% CI: 0.70-1.23; p=0.61) and all-cause mortality (HR 1.48, 95% CI: 1.09-2.01; p=0.013 and HR 0.90, 95% CI: 0.63-1.30; p=0.58) compared to patients without AF (Table 2). The risk for ischaemic stroke was higher in patients with new AF, but the association lacked statistical significance after multivariable adjustment (subdistribution HR [sHR] 1.66, 95% CI: 0.81-3.38; p=0.16). A sensitivity analysis leaving out patients who underwent CABG during admission yielded similar results, but with a stronger trend towards an increased risk of ischaemic stroke in new AF patients in the adjusted subdistribution hazard analysis (sHR 2.21, 95% CI: 0.98-4.95; p=0.056) (Supplementary Table 1). The full multivariable models are reported in Supplementary Table 2, Supplementary Table 3,Supplementary Table 4,Supplementary Table 5, Supplementary Table 6,Supplementary Table 7, Supplementary Table 8,Supplementary Table 9.
The Kaplan-Meier curve (Central illustration) showed the greatest divergence in MACE during the first 30 days. Closer inspection of 30-day outcomes showed that the worst outcomes of new AF regarding MACE were mainly driven by all-cause mortality and ischaemic stroke, but not by MI (Supplementary Figure 1).
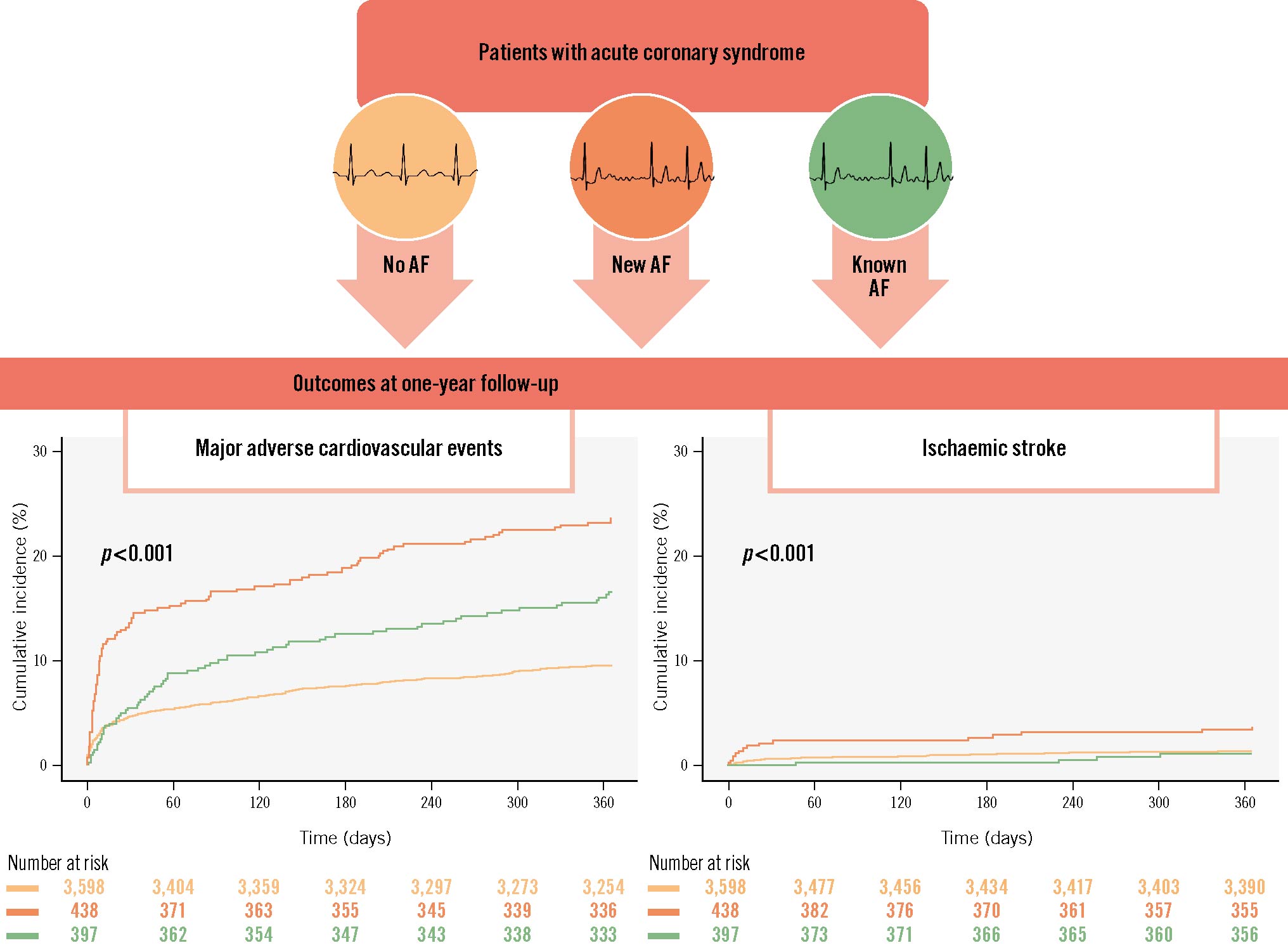
Central illustration. Incidence curves of major adverse cardiovascular events and ischaemic stroke in ACS patients according to AF status. ACS: acute coronary syndrome; AF: atrial fibrillation
CHARACTERISTICS OF NEW ATRIAL FIBRILLATION EPISODES AND THEIR ASSOCIATION WITH CLINICAL OUTCOMES
The duration of new AF episodes was longer than 24 hours in 44.4% of patients (Figure 2). Of all new AF cases, 37.8% occurred post-CABG. Of these post-CABG cases, 92.7% occurred more than 24 hours after ACS presentation. The duration of new AF emerging post-CABG was short (less than 24 hours) in 54.2% of the cases. The onset of AF episodes was early after ACS presentation (within 24 hours) in 69.4% of non-CABG patients.
A longer duration of a new AF episode was associated with increased MACE (HR 1.99, 95% CI: 1.36-2.93; p<0.001), all-cause mortality (HR 1.97, 95% CI: 1.25-3.10; p=0.004), and a trend towards increased ischaemic stroke (sHR 2.57, 95% CI: 0.88-7.47; p=0.08) (Figure 2). The timing of the onset of the AF episode showed no significant association with clinical outcomes; however, there was a trend towards increased MACE with episodes starting >24 hours after presentation (HR 1.53, 95% CI: 0.98-2.38; p=0.06). Episodes of new AF that occurred post-CABG, on the other hand, were associated with lower MACE (HR 0.52, 95% CI: 0.31-0.86; p=0.012) and all-cause mortality (HR 0.44, 95% CI: 0.23-0.83; p=0.012), as compared to new AF that occurred spontaneously after ACS.
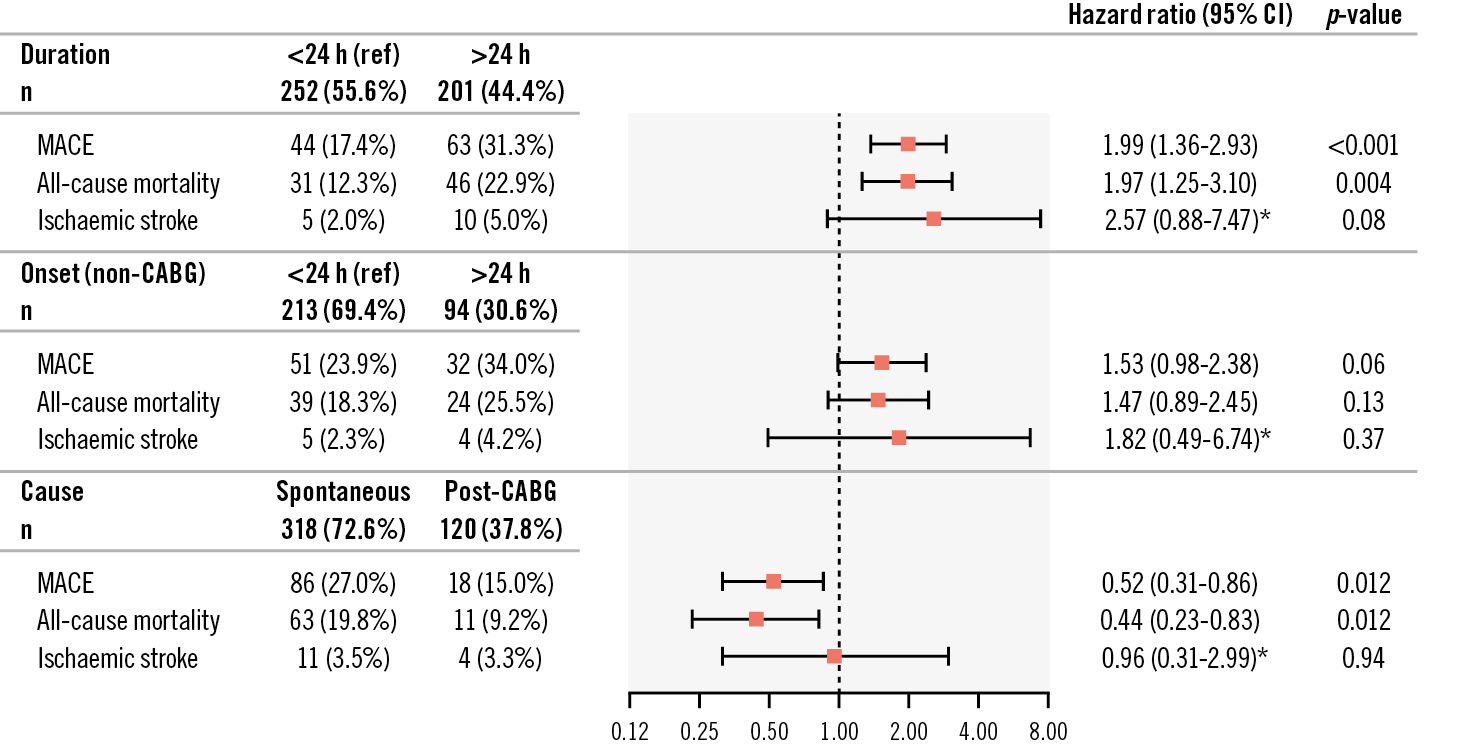
Figure 2. Association of new AF episode characteristics with adverse outcomes. New AF episodes lasting over 24 hours are associated with an increased risk of MACE. New AF episodes with onset beyond 24 hours after ACS show a trend towards worse outcomes. New AF episodes occurring post-CABG are associated with a decreased risk of MACE. *Subdistribution hazard ratio. ACS: acute coronary syndrome; AF: atrial fibrillation; CI: confidence interval; CABG: coronary artery bypass graft; MACE: major adverse cardiovascular events
PRESCRIPTION OF ORAL ANTICOAGULANTS ACCORDING TO ATRIAL FIBRILLATION TYPE AND EPISODE CHARACTERISTICS
OAC use prior to admission was 2.6% amongst patients without AF, 5.3% amongst patients with new AF, and 83.1% amongst patients with known AF (Figure 3). Prescription rates of OAC at discharge were 5.0%, 53.5%, and 89.2%, respectively. The rates of self-reported OAC use at 1 month were 5.9%, 52.2%, and 86.7%, respectively. At 1 year, those rates were 7.4%, 52.2%, and 87.3%, respectively.
Patients with newly diagnosed atrial fibrillation who were prescribed OAC at discharge were less frequently prescribed aspirin than patients not receiving OAC (31.6% vs 98.4%; p<0.001). For combination therapy with OAC, clopidogrel was more frequently chosen than the potent P2Y12 inhibitors ticagrelor or prasugrel (76.3% vs 14.0%) (Table 3).
In new AF patients with a CHA2DS2-VASc score of 1, OAC prescription at discharge was 29.7%, and in new AF patients with a CHA2DS2-VASc score ≥2, it was 57.4%. OAC prescription in patients with new AF was significantly higher if the episode lasted longer than 24 hours (42.6% vs 72.3%; p<0.001), but lower in patients who had undergone CABG during admission versus those who did not undergo CABG (34.0% vs 61.7%; p<0.001). OAC prescription did not differ (58.2% vs 50.0%; p=0.14) between patients with early (<24 hours) or late (>24 hours) onset of new AF.
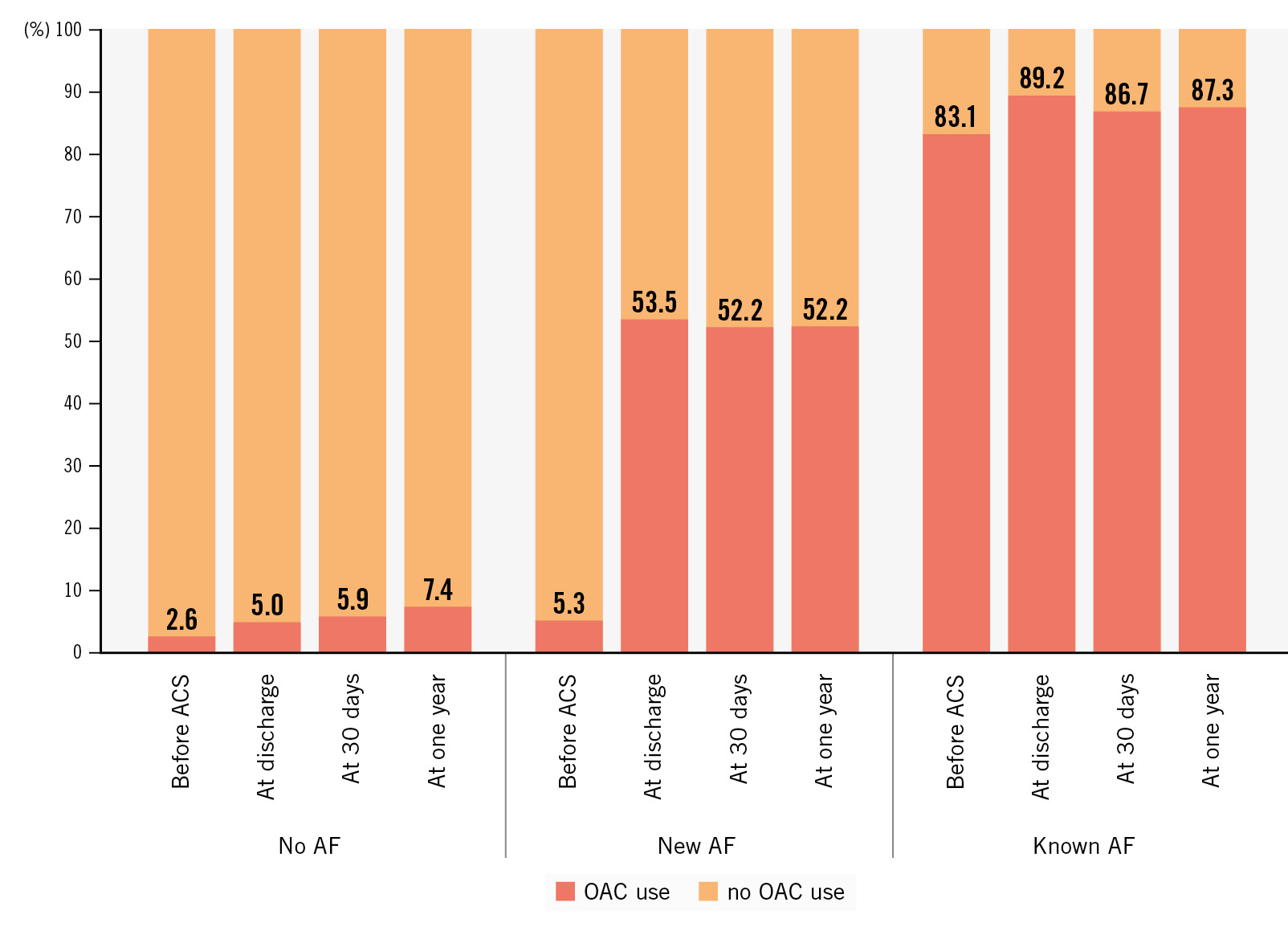
Figure 3. OAC use over time according to AF status. ACS: acute coronary syndrome; AF: atrial fibrillation; OAC: oral anticoagulants
Table 2. Crude and adjusted outcomes of ACS patients according to AF status.
| New AF | ||||||
|---|---|---|---|---|---|---|
| Crude HR | Adjusted HR* | |||||
| No AF | New AF | HR (95% CI) | p-value | HR (95% CI) | p-value | |
| MACE | 346 (9.6) | 104 (23.7) | 2.70 (2.17-3.36) | <0.001 | 1.52 (1.19-1.90) | <0.001 |
| All-cause mortality | 174 (4.8) | 74 (16.9) | 3.73 (2.84-4.90) | <0.001 | 1.48 (1.09-2.01) | 0.013 |
| Ischaemic stroke | 45 (1.3) | 15 (3.4) | 2.77 (1.55-4.98)** | <0.001 | 1.66 (0.81-3.38)** | 0.16 |
| Myocardial infarction | 159 (4.4) | 22 (5.0) | 1.14 (0.73-1.79)** | 0.56 | 1.15 (0.72-1.86)** | 0.56 |
| Known AF | ||||||
| Crude HR | Adjusted HR* | |||||
| No AF | Known AF | HR (95% CI) | p-value | HR (95% CI) | p-value | |
| MACE | 346 (9.6) | 66 (16.6) | 1.77 (1.36-2.30) | <0.001 | 0.93 (0.70-1.23) | 0.61 |
| All-cause mortality | 174 (4.8) | 40 (10.1) | 2.13 (1.51-3.00) | <0.001 | 0.90 (0.63-1.30) | 0.58 |
| Ischaemic stroke | 45 (1.3) | 4 (1.0) | 0.80 (0.29-2.22)** | 0.67 | 0.48 (0.16-1.46)** | 0.19 |
| Myocardial infarction | 159 (4.4) | 25 (6.3) | 1.43 (0.94-2.18)** | 0.09 | 0.96 (0.60-1.54)** | 0.87 |
| Data are presented as n (%). P-values in bold indicate statistical significance. *Adjusted for age, smoking, hypertension, prior myocardial infarction, prior percutaneous coronary intervention, prior coronary artery bypass graft, prior stroke, peripheral artery disease, type of ACS at admission, Killip class at admission, out-of-hospital cardiac arrest at admission, left ventricular ejection fraction, number of diseased coronary vessels, coronary artery bypass graft during admission, and renal function. **Subdistribution hazard ratio. ACS: acute coronary syndrome; AF: atrial fibrillation; CI: confidence interval; HR: hazard ratio; MACE: major adverse cardiovascular events | ||||||
OUTCOMES OF NEW ATRIAL FIBRILLATION PATIENTS ACCORDING TO EPISODE CHARACTERISTICS AND ORAL ANTICOAGULANT TREATMENT
The prescription of OAC was a significant effect modifier on the association of new AF with MACE (pinteraction=0.041). Therefore, this interaction was further explored.
An extensive comparison of baseline characteristics between new AF patients discharged with or without OAC is provided in Table 3. Patients with new AF that were discharged on OAC had significantly more comorbidities that may predispose to stroke, as expressed by their higher CHA2DS2-VASc scores (mean 3.8 vs 3.2; p<0.001).
Kaplan-Meier curves comparing the clinical outcomes of patients with new AF discharged with or without OAC are shown in Figure 4. MACE and ischaemic stroke rates were numerically higher in patients treated with OAC (14.4% vs 11.2% and 2.3% vs 1.6%;p>0.05 for both). After adjustment for baseline imbalances, there was no difference in MACE between the groups (adjusted HR 0.93, 95% CI: 0.52-1.65; p=0.80) (Supplementary Table 10). Bleeding events, however, were significantly higher in patients treated with OAC (adjusted sHR 1.56, 95% CI: 1.06-2.29; p=0.026). Major bleeding events occurred in 2.7% of patients without and 6.0% of patients with OAC.
After excluding new AF episodes that occurred post-CABG, outcomes including ischaemic stroke were incrementally worse starting in patients with short episodes occurring early during an ACS event up to patients with long episodes with late onset (>24 hours after ACS), despite higher rates of OAC treatment in the higher-risk categories (Figure 5). The risk of ischaemic stroke in patients with a short episode of early-onset new AF was not significantly increased as compared to patients without AF (0.0% vs 1.3%; p=0.21). All other groups of new AF episodes during ACS, however, were accompanied by an increased risk of ischaemic stroke (3.8-7.5%; p<0.05).
Table 3. Clinical characteristics of ACS patients with new AF according to OAC treatment at discharge.
| No OAC n=187 | OAC n=215 | p-value | % missing | |
|---|---|---|---|---|
| Demographics and cardiovascular risk factors | ||||
| Age, years | 68±12 | 74±9 | <0.001 | 0.0 |
| Female sex | 33 (17.6) | 63 (29.3) | 0.009 | 0.0 |
| Body mass index, kg/m² | 26.9±4.0 | 27.5±4.5 | 0.17 | 3.4 |
| Hypertension | 116 (62.0) | 130 (60.7) | 0.87 | 0.7 |
| Hypercholesterolaemia | 101 (55.8) | 134 (64.7) | 0.09 | 3.6 |
| Diabetes mellitus | 47 (25.1) | 51 (23.9) | 0.87 | 0.7 |
| Active smoker | 53 (28.6) | 44 (20.8) | 0.09 | 2.3 |
| Medical history | ||||
| Myocardial infarction | 35 (18.8) | 42 (19.5) | 0.96 | 0.2 |
| PCI | 30 (16.0) | 38 (17.7) | 0.76 | 0.0 |
| CABG | 9 (4.8) | 20 (9.3) | 0.12 | 0.0 |
| Stroke | 17 (9.1) | 34 (15.8) | 0.06 | 0.0 |
| Peripheral artery disease | 14 (7.5) | 33 (15.3) | 0.022 | 0.0 |
| Congestive heart failure | 10 (5.3) | 6 (2.8) | 0.29 | 0.0 |
| Clinically relevant bleeding | 11 (5.9) | 17 (8.0) | 0.54 | 1.1 |
| Laboratory | ||||
| Haemoglobin, mmol/L | 8.6±1.1 | 8.5±1.2 | 0.53 | 0.9 |
| Platelet count, 109/L | 250±85 | 247±81 | 0.70 | 2.1 |
| eGFR, mL/min | 73±24 | 68±21 | 0.017 | 0.0 |
| ACS presentation | ||||
| Discharge diagnosis | 0.003 | 0.0 | ||
| UAP | 10 (5.3) | 10 (4.7) | ||
| NSTEMI | 69 (36.9) | 108 (50.2) | ||
| STEMI | 9 (4.8) | 20 (9.3) | ||
| Semirecent infarction | 99 (52.9) | 77 (35.8) | ||
| Killip class upon admission | 0.006 | 0.0 | ||
| I | 158 (84.5) | 163 (75.8) | ||
| II | 16 (8.6) | 43 (20.0) | ||
| III | 3 (1.6) | 4 (1.9) | ||
| IV | 10 (5.3) | 5 (2.3) | ||
| Out-of-hospital cardiac arrest | 25 (13.4) | 10 (4.7) | 0.004 | 0.0 |
| Number of diseased coronary vessels | 0.012 | 10.7 | ||
| 0 | 1 (0.6) | 10 (5.2) | ||
| 1 | 45 (26.0) | 65 (34.0) | ||
| 2 | 49 (28.3) | 45 (23.6) | ||
| 3 | 78 (45.1) | 69 (36.1) | ||
| Graft dysfunction | 0 (0.0) | 2 (1.0) | ||
| CK max, U/L | 1,535±4,032 | 1,340±2,132 | 0.55 | 5.7 |
| CABG during admission | 81 (43.3) | 56 (26.0) | <0.001 | 0.0 |
| CHA2DS2-VASc score | 3.2±1.5 | 3.8±1.4 | <0.001 | 0.0 |
| LVEF | 0.47 | 4.1 | ||
| >50% | 109 (60.9) | 117 (56.2) | ||
| 30-50% | 54 (30.2) | 65 (31.2) | ||
| <30% | 16 (8.9) | 26 (12.5) | ||
| Antithrombotic medication at discharge | ||||
| Aspirin | 184 (98.4) | 68 (31.6) | <0.001 | 0.0 |
| Clopidogrel | 58 (31.2) | 164 (76.3) | <0.001 | 0.2 |
| Ticagrelor or prasugrel | 117 (62.9) | 30 (14.0) | <0.001 | 0.2 |
| Data are presented as mean±SD or n (%). P-values in bold indicate statistical significance. ACS: acute coronary syndrome; AF: atrial fibrillation; CABG: coronary artery bypass graft; CAD: coronary artery disease; CK: creatine kinase; eGFR: estimated glomerular filtration rate; LVEF: left ventricular ejection fraction; NSTEMI: non-ST-segment elevation myocardial infarction; OAC: oral anticoagulants; PCI: percutaneous coronary intervention; SD: standard deviation; STEMI: ST-segment elevation myocardial infarction; UAP: unstable angina pectoris | ||||
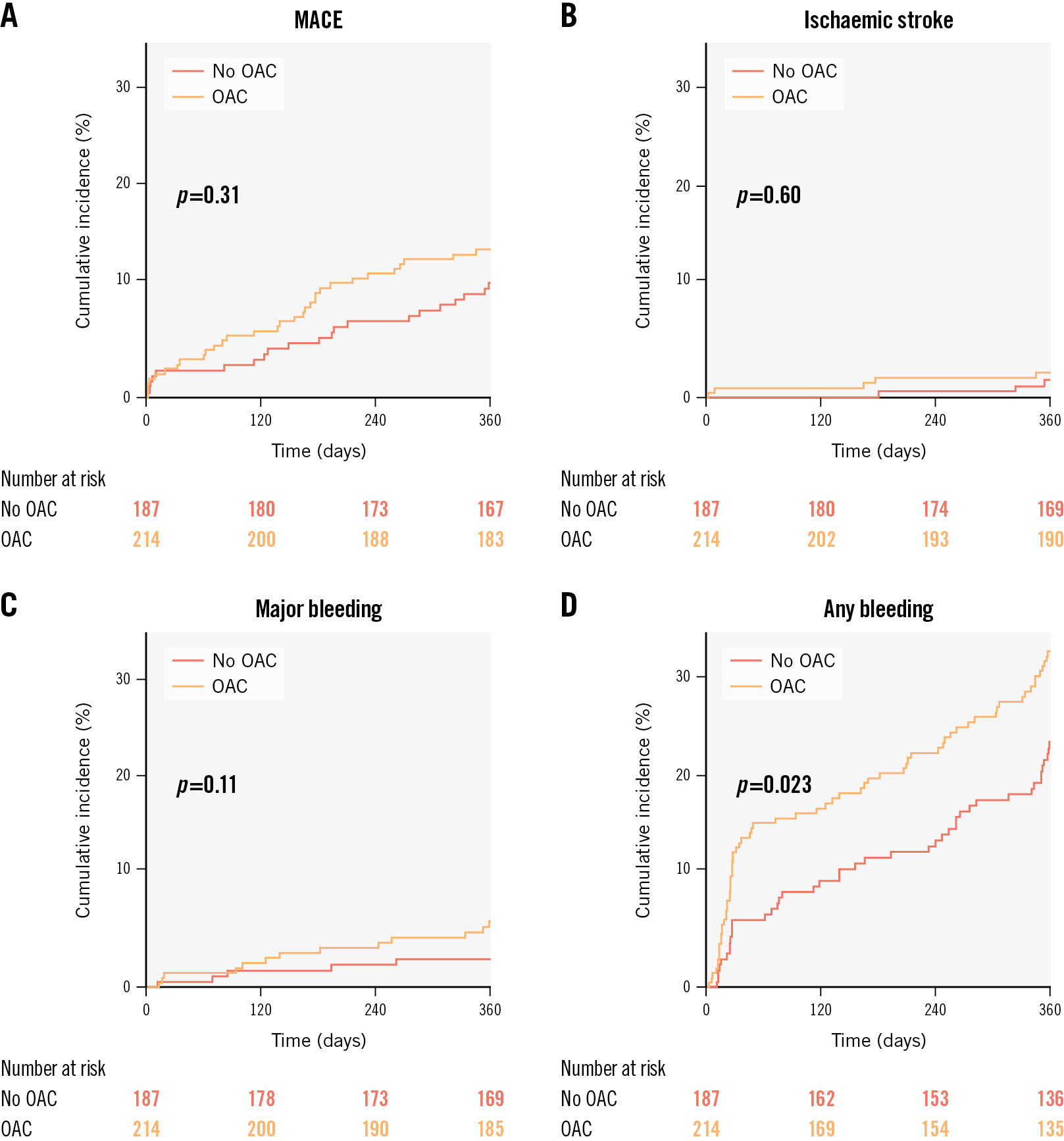
Figure 4. Clinical outcomes in new AF patients according to OAC treatment at discharge. AF: atrial fibrillation; MACE: major adverse cardiovascular events; OAC: oral anticoagulants
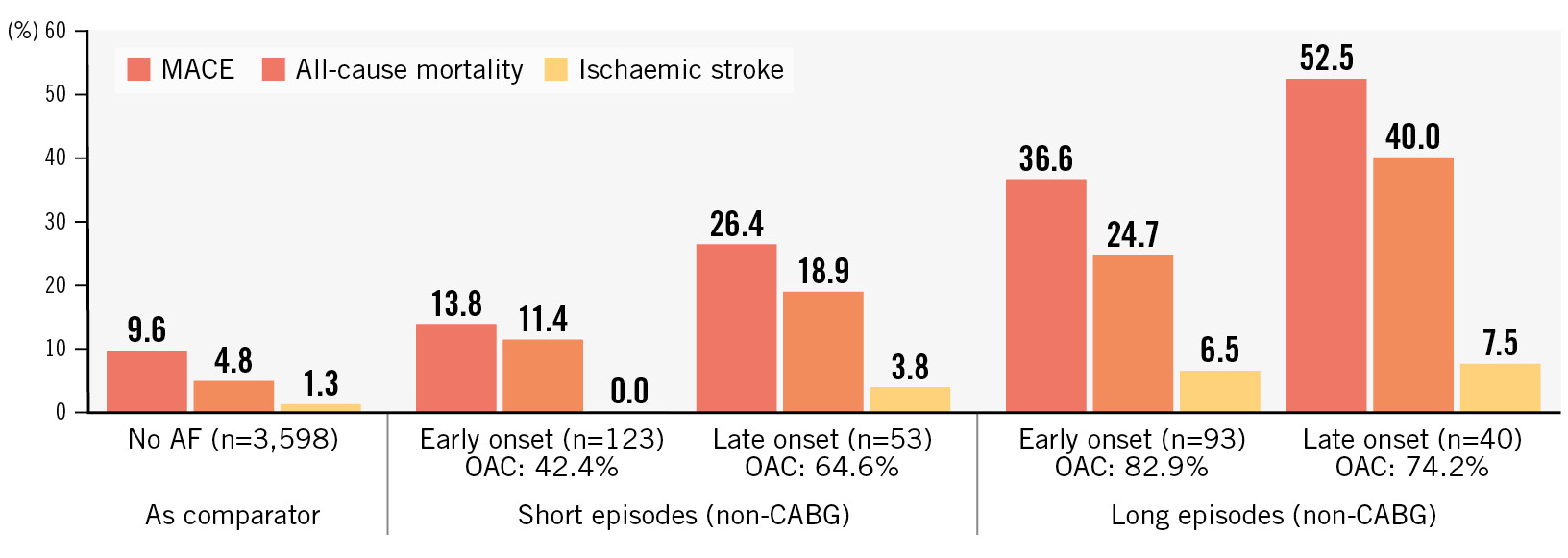
Figure 5. Adverse events according to new AF onset and duration. Early onset: within 24 hours after presentation; late onset: more than 24 hours after presentation; short episode: under 24 hours; long episode: over 24 hours. AF: atrial fibrillation; CABG: coronary artery bypass graft; MACE: major adverse cardiovascular events; OAC: oral anticoagulants
Discussion
In this study, we found that ACS patients who develop new AF during admission show worse outcomes regarding MACE than patients without AF or with known AF. The association of new AF with an increased risk of ischaemic stroke lost statistical significance after adjusting for confounders, but sensitivity analysis leaving out patients that underwent CABG during index admission yielded near-significant results (sHR 2.21, 95% CI: 0.98-4.95; p=0.056) (Supplementary Table 1). The more pronounced, independently increased risk of new AF in patients without CABG seems in line with the observation in our manuscript that post-CABG new AF is associated with a less pronounced risk of MACE and ischaemic stroke compared to spontaneously occurring new AF in ACS patients. Furthermore, longer-lasting episodes (>24 hours) were associated with poorer outcomes. Around half of patients newly diagnosed with AF were discharged on OAC therapy, whereas over 90% of patients with known AF were treated with OAC. We found no significant benefit of OAC in patients with new AF; however, this is likely due to the limitations of the observational nature of this study. OAC treatment rates amongst new AF patients were higher in patients with features associated with increased MACE and ischemic stroke, such as CHA2DS2-VASC ≥2 and AF episodes lasting >24 hours.
The association of AF with worse outcomes in ACS patients is known and has been reported previously1314. The co-occurrence of these two diseases can aggravate each other and seem to form a vicious cycle15. The fact that patients with AF show worse outcomes than those without AF may, in part, be explained by more extensive cardiovascular disease. In fact, the incidence of comorbidities in our study gradually increased from patients without, to patients with new and, finally, known AF.
The finding that new AF patients show worse outcomes than patients with known AF, however, is surprising and seems counterintuitive. From the results of this study, we hypothesise two explanations for these findings.
First, patients with new AF presented with larger infarctions with more haemodynamic impact. This is illustrated by the greater number of patients with new AF presenting at the index ACS with Killip class III/IV or OHCA; they had higher maximum CK values, and presented more frequently with semirecent MI, i.e., a late presentation with MI for which reperfusion therapy was too late. As a result, patients with new AF had lower LVEF at discharge than patients without AF or with known AF. This is known to be associated with heart failure and worse prognosis in ACS patients16.
Second, patients with new AF were less often treated with OAC: at discharge 54.7% were prescribed OAC versus 90.6% of known AF patients. Although current guidelines do not specifically state that all ACS patients with new AF should be treated with OAC, it recommends OAC treatment in patients with a CHA2DS2-VASc score ≥2. In this study, most patients had a CHA2DS2-VASc score ≥2 (mean 3.6, range 1-8). Therefore, according to the guidelines, almost all patients with new AF should have been treated with OAC. The undertreatment of new AF suggests uncertainty as to whether OAC is warranted for stroke reduction in those patients. However, in this study we found that not only MACE but also stroke as a separate component of MACE was increased with new AF. The risk of ischaemic stroke was not increased for patients with known AF. While patients with known AF were treated with OAC in >90% of cases, patients with new AF were treated in only half of cases. Therefore, we speculate that the excess stroke risk in new AF patients may (at least, in part) have been ameliorated with more adequate OAC treatment. However, we also noted a higher bleeding risk with the use of OAC therapy. Therefore, the balance may tilt towards no OAC treatment in those patients with increased risk of major bleeding as well as in patients with a more “benign” ischaemic phenotype of AF.
For instance, AF occurring post-CABG seems to have a lower risk of thromboembolic events compared to spontaneously occurring AF in ACS patients in this research. Still, a MACE rate of 15.0%, mortality rate of 9.2%, and stroke rate of 3.3% in post-CABG new AF are higher than the rates in patients without AF and are more similar to other patients with new AF (Table 2). This increased risk of stroke might encourage the use of OAC therapy; however, aetiologies other than AF may also play a role in the post-CABG population17. The currently ongoing Anticoagulation for New-Onset Post-Operative Atrial Fibrillation After CABG (PACES) randomised controlled trial (ClinicalTrials.gov: NCT04045665) will hopefully soon elucidate on the added value of OAC therapy in patients with new onset AF after CABG. This trial randomises patients that develop new AF within a week after CABG to OAC therapy versus single antiplatelet therapy.
Similarly, our study suggests that the risk of ischaemic stroke in patients with a short paroxysm of new AF is limited. Two other reports, however, showed that paroxysmal AF that converted to sinus rhythm before discharge was also associated with increased risk of ischaemic stroke1819. This is in line with other studies that show recurrent AF after discharge in a high proportion of patients with a paroxysm of new AF during ACS: new AF during ACS is not transient in many cases but recurrent1820. Moreover, recurrent episodes may be missed in outpatient follow-up, as it is silent in many cases, which hampers treatment and may worsen patient outcomes21. Therefore, these results from our study should be interpreted with caution and not necessarily discourage OAC prescription for patients with only a short paroxysm of new AF.
Of note, the temporal distribution of excess ischaemic stroke in patients with newly diagnosed AF showed a remarkable clustering within the first 30 days. This research evaluated the association of (undertreated) newly diagnosed atrial fibrillation as the aetiology of MACE or, more specifically, ischaemic stroke, after an ACS. However, other aetiologies may play a role in the occurrence of stroke, such as a complication of a PCI or CABG procedure in the setting of ACS. Second, stroke due to left ventricular thrombi may play a role in large MI with regional wall akinesia and dyskinesia, as this may result in blood stasis, inflammatory changes, and hypercoagulability22.
Limitations
Our study provides a detailed description of a large cohort of ACS patients that were categorised as having no, known, or new AF during ACS hospitalisation. As we manually reviewed all available ECGs of these 4,433 patients, our study is more precise than studies relying on, e.g., International Classification of Diseasese (ICD) codes or discharge medication, as short episodes may not be registered and thus missed with those methods. Furthermore, we characterised the episodes according to onset, duration and post-CABG occurrence, which are the main factors that clinicians may take into account for treatment decisions. Thanks to the extensive patient characteristics collected in the FORCE-ACS registry, which was the basis of this study, we were able to adjust for detailed baseline differences. Also, data regarding medication use and events during follow-up were of high quality, as they were both patient-reported and verified in the patient files by the study team.
Our study also has some limitations. The occurrence of new post-discharge AF was not reported, which may have been interesting to study in relation to clinical outcomes, especially in patients with newly diagnosed AF. Furthermore, the observational nature of this study limits us in concluding whether or not to prescribe OAC for new AF patients. However, as no randomised studies yet exist for new AF in ACS patients, we believe this contributes to the best available evidence on this subject.
Conclusions
In patients with ACS, newly diagnosed AF was associated with worse outcomes regarding MACE and ischaemic stroke. Among patients with new AF, episodes lasting >24 hours were associated with worse outcomes than shorter episodes, and post-CABG episodes showed relatively better outcomes than spontaneously occurring new AF. Only half of new AF patients were discharged on OAC therapy versus >90% with known AF.
Impact on daily practice
Newly diagnosed atrial fibrillation (AF) in patients with acute coronary syndrome (ACS) is associated with an increased risk of major adverse cardiovascular events and stroke, unlike known AF. Oral anticoagulants are prescribed in only half of patients with newly diagnosed AF during an ACS. These results underscore the need to consider oral anticoagulants in all patients with newly diagnosed AF during an ACS.
Funding
The FORCE-ACS registry is supported by a grant from ZonMw, the St. Antonius Research Fund, and AstraZeneca.
Conflict of interest statement
J.M. ten Berg reports an institutional grant from Daiichi Sankyo; consulting fees from CeleCor; and speaker fees from Daiichi Sankyo and CeleCor. The other authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
