Mild-to-moderate aortic regurgitation (AR) after transcatheter aortic valve implantation (TAVI) is common and often clinically silent. Higher-degree AR may occur, with significant haemodynamic and clinical consequences. Treatment of this condition is challenging and there are no evidence-based therapeutic options. This image illustrates the successful percutaneous management of clinically relevant paravalvular leaks (PVL) after implantation of the CoreValve bioprosthesis (Medtronic, Minneapolis, MN, USA) with the use of vascular plug devices.
Conflict of interest statement
The authors report no financial relationships or conflicts of interest regarding the content herein.
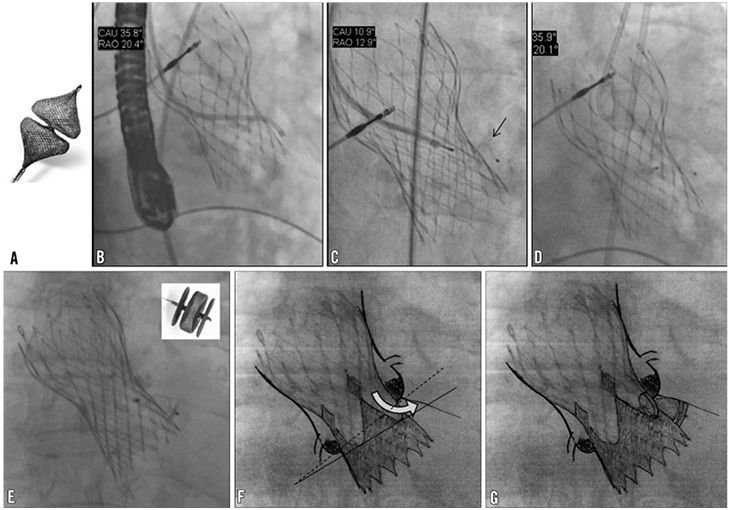
Figure 1. Examples of successful percutaneous closure of severe paravalvular leak (PVL) after transcatheter aortic valve implantation (TAVI) using two different Amplatzer™ vascular plug (AVP) devices (St. Jude Medical, St. Paul, MN, USA). A) The Amplatzer™ Vascular Plug 4. B) The frame of the bioprosthesis was crossed using an Amplatz Left diagnostic catheter, with the help of a hydrophilic wire. C) Catheter exchange into the left ventricle was performed with a 260 cm hydrophilic wire, and a 6 mm device was advanced through a 6 Fr multipurpose PCI catheter. The distal part of the AVP4 device is visible (arrow). D) Position of the device across the valve frame after its release. E) Closure of a PVL with an AVP2 device (box). The device was released with the proximal disc within the aortic side of the frame and the other two lobes sitting below the severely calcified native valve annulus. F and G) Drawings superimposed on the angiography to highlight the mechanism and the site of aortic regurgitation (F) and the position of the vascular plug (G). The lines show the presence of an angle between the aortic annulus plane (dotted line) and the bioprosthetic valve plane (solid line).
