A 75-year-old woman was referred to our centre for management of a symptomatic (New York Heart Association [NYHA] Class III) severe (effective regurgitant orifice area: 44 mm²) secondary mitral regurgitation (MR). She had no previous medical history except for a dual-chamber pacemaker implantation for high-grade atrioventricular block two years earlier. Her Society of Thoracic Surgeons (STS) score was 4.0% and left ventricular ejection fraction was 55%. Owing to her frailty, the Heart Team recommended transcatheter management of this MR. Because of severe leaflet restriction and short length (6 mm) of the posterior leaflet (Figure 1A, Figure 1B), we considered a mitral valve replacement rather than a transcatheter edge-to-edge repair (TEER). A self-expanding bioprosthetic valve (Tendyne [Abbott]), was successfully deployed transapically via a left lateral thoracotomy with a good outcome. The 3-month follow-up found an asymptomatic patient, treated with Coumadin, with no residual MR (Moving image 1), a transprosthetic gradient of 2 mmHg, and a mild tricuspid regurgitation (TR).
At follow-up, successive echocardiography explorations highlighted worsening TR. Four years after the Tendyne implantation, the patient was once again symptomatic (NYHA Class II, with fatigability and asthaenia, lower extremity oedema) because of a severe secondary TR (Figure 1C, Moving image 2). Her systolic pulmonary artery pressure was 29 mmHg. The echocardiographic parameters of the Tendyne valve were stable and no hypoattenuated leaflet thickening (HALT) was observed on computed tomograph. In addition to a tricuspid annulus dilatation (“atrial TR”), a careful assessment of the tricuspid valve showed a major restriction of the septal leaflet due to the pacemaker ventricular lead (“pacemaker-related TR”) (Moving image 3), suggesting the unfeasibility of a tricuspid TEER. The STS score and TRI-SCORE were 8.6% and 5/12, respectively, LVEF was 40%, and right ventricular function was preserved. Thus, we implanted a self-expanding bioprosthetic valve (LuX-Valve [Jenscare]), using a transjugular approach, with a favourable outcome (Moving image 4). At 6 months, the patient had no further symptoms (NYHA Class I), with no mitral or tricuspid regurgitation (Figure 1D, Moving image 5, Moving image 6) and no argument for pacemaker ventricular lead damage.
In the management of symptomatic severe mitral and tricuspid regurgitations, TEER is usually considered as the first option for patients who are ineligible for surgery. However, valve replacement is a promising treatment, especially when the expected results of TEER would be unacceptable1.
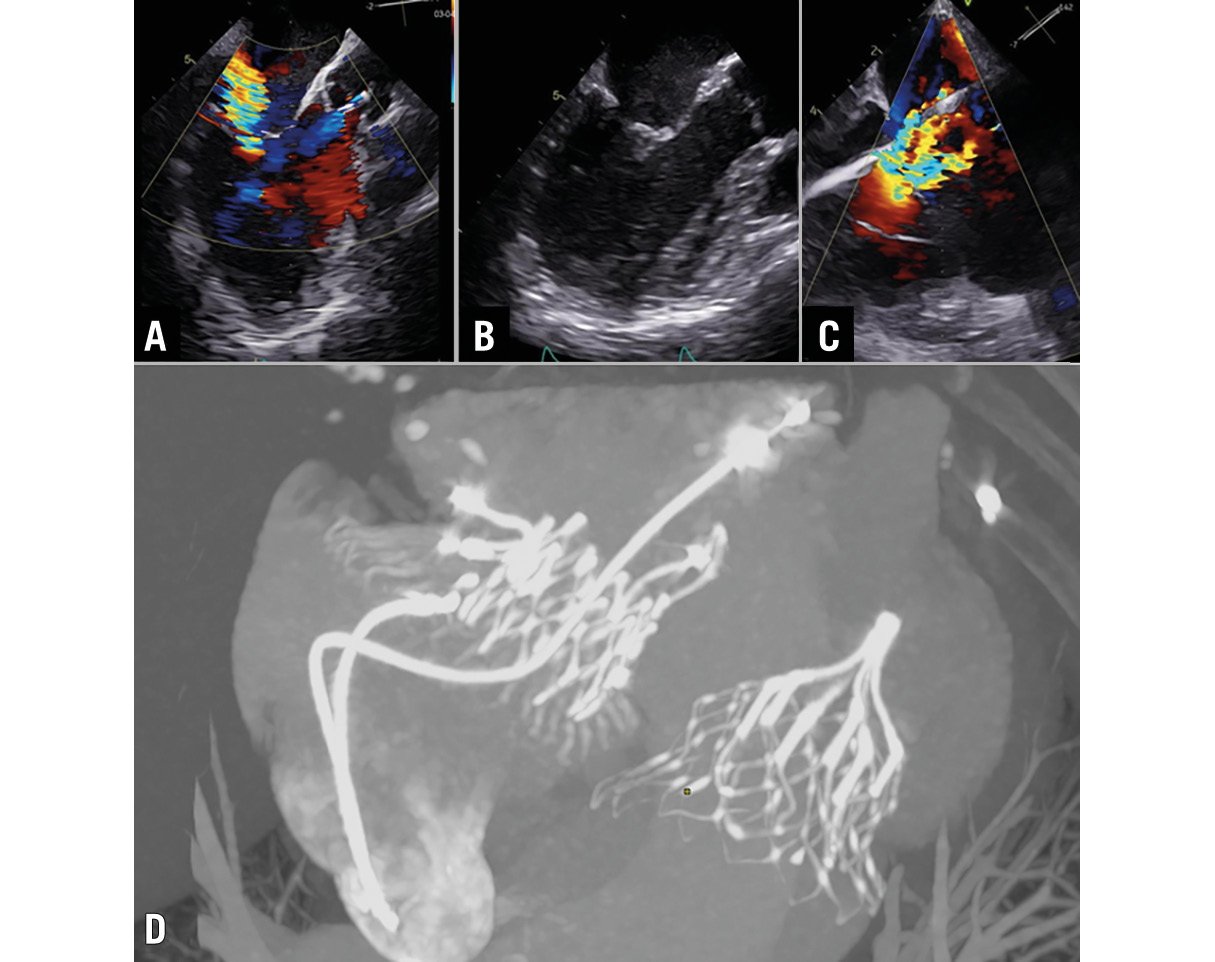
Figure 1. Multimodal assessment of a mitral and tricuspid regurgitation successfully treated by a double transcatheter replacement. A, B) Transoesophageal echocardiogram showing a severe secondary mitral regurgitation, with a short and very restrictive posterior leaflet. C) Transoesophageal echocardiogram showing a severe atrial and pacemaker-related tricuspid regurgitation. D) Computed tomography angiogram of the LuX-Valve (Jenscare) and the Tendyne valve (Abbott).
Conflict of interest statement
G. Leurent reports speaker, proctoring activity and consultant fees from Abbott and Edwards Lifesciences. A. Anselmi reports proctoring activity for Abbott. V. Auffret reports speaker fees from Edwards Lifesciences and Medtronic; and consultant fees from Medtronic and Boston Scientific. The other authors have no conflicts of interest related to the topic to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Transoesophageal echocardiogram showing no intra- or paraprosthetic mitral regurgitation.
Moving image 2. Transthoracic echocardiogram showing severe tricuspid regurgitation and no residual mitral regurgitation.
Moving image 3. Transoesophageal echocardiogram showing a major restriction of the septal leaflet of the tricuspid valve due to the pacemaker ventricular lead.
Moving image 4. Transthoracic echocardiogram showing no intra- or paraprosthetic tricuspid regurgitation.
Moving image 5. Transthoracic echocardiogram showing no residual mitral or tricuspid regurgitation.
Moving image 6. Cine computed tomography angiogram of the LuX-Valve and the Tendyne valve.
