Cory:
Unlock Your AI Assistant Now!
With the publication of several large randomised clinical trials (RCT), intracoronary imaging-guided percutaneous coronary intervention (PCI) was a well-covered topic in 20231234. In general, these studies confirmed the benefit of the application of both sound- (intravascular ultrasound [IVUS]) and light- (optical coherence tomography [OCT] or optical frequency domain imaging [OFDI]) based intracoronary imaging systems. The most important benefits are seen in the most challenging PCI cases, such as in patients with coronary bifurcation lesions2.
In this issue of EuroIntervention, Otake et al report the results of the OPINION ACS randomised controlled trial, a comparison of OFDI- vs IVUS-guided PCI in the specific subset of patients presenting with an acute coronary syndrome (ACS)5. With a total of 158 patients enrolled, the current study is much smaller than other recently reported trials in this field (e.g., ILUMIEN IV: 2,487 patients; OCTIVUS: 2,008 patients; RENOVATE COMPLEX PCI: 1,639 patients; OPINION: 829 patients; OCTOBER: 1,201 patients)12346. It is also not the first report on intracoronary imaging in ACS patients, as more than half of patients in ILUMIEN IV, RENOVATE COMPLEX PCI and OCTOBER and almost a quarter of those in OCTIVUS presented with an ACS when qualifying for inclusion in these studies.
The conclusion of OPINION ACS is that OFDI-guided PCI is non-inferior to IVUS-guided PCI, which is completely in line with the results from the much larger studies described above. The specific value of the current report lies in the details it provides with respect to the methodology of the preimplantation stent sizing algorithm and its direct effect on the intracoronary imaging endpoints obtained immediately after implantation and at later follow-up.
In fact, the results from the OPINION ACS study appear to challenge the widely adopted concept of vessel-based stent sizing. Going back to 2017, the authors of the current report published the landmark OPINION study, the first large RCT comparing OFDI- vs IVUS-guided PCI in an all-comers patient population6. This study was the first to prove the non-inferiority of OFDI- versus IVUS-guided PCI, with excellent clinical and angiographic outcomes in both imaging-guided intervention arms.
It is important to mention that the OPINION investigators use a lumen-based strategy for stent sizing in the OFDI-guided arm of their studies. The mean lumen diameter in a normal distal landing zone is measured and rounded up to the next stent size (up to 0.25 mm larger). This contrasts with the vessel-sizing methodology used in the OCT-guided arms in the ILUMIEN III and IV randomised trials as well as several other studies in the field. In this latter algorithm, when >180° of external elastic lamina (EEL) can be discriminated at the distal reference area, an EEL-EEL measurement is performed, and this value is rounded down to the next stent size (up to 0.25 mm smaller). Comparable measurements at the proximal landing zone are then used for determining appropriate post-dilatation balloon sizes. As a consequence, with vessel-based stent-sizing algorithms, larger stent sizes are usually chosen, resulting in larger post-implantation minimum stent area (MSA) values. Stent underexpansion has been defined as a major risk factor for stent failure, and as a consequence, optimising stent expansion is now considered the most important goal of imaging-guided interventions7.
In the imaging substudy of the original OPINION trial, the authors provided additional information on the differential effect of a lumen (OFDI group) versus a vessel (IVUS group) stent-sizing algorithm, which indeed dictated a slightly, but significantly, smaller stent diameter in the OFDI-guided group than in the IVUS-guided group. Not surprisingly, in the OFDI-guided arm, there was a trend towards a smaller MSA after PCI than with the IVUS-based strategy8.
This difference is usually not observed when a vessel-based stent-sizing algorithm is used in both the OCT and IVUS arms, such as in the ILUMIEN III study9. This has resulted in the perception that choosing larger sized stents in OCT-guided procedures improves outcomes and has led to the widespread adoption of vessel-based sizing in OCT-guided PCI protocols.
However, the detailed imaging data in the current report by Otake et al to some extent question this widespread belief5. Apart from a trend towards a smaller MSA immediately after stent implantation, proximal edge dissection and irregular protrusion were significantly less frequent in OFDI-guided procedures than in IVUS-guided procedures. Strikingly, the difference in MSA immediately post-procedure did not translate into a difference in minimum lumen area (MLA) at the 8-month follow-up angiography and OFDI assessment due to a trend towards a smaller average neointima area in the OFDI-guided group (Figure 1). In this respect, these results are a confirmation of the earlier reported findings of the OPINION Imaging substudy8. In other words, an OCT-guided strategy − as used in OPINION ACS − does result in smaller stent sizes than an IVUS-guided strategy, but it provokes less neointima formation, ultimately leading to very comparable luminal areas at follow-up.
The currently reported imaging data by Otake et al remind us that we should be cautious with respect to the potential risks associated with overaggressive vessel dilatation. Indeed, irregular protrusions through the struts − identified by OCT after aggressive stenting − is an independent predictor of 1-year device-oriented clinical endpoints, in particular, target lesion revascularisation10. Immediately after stent implantation, a higher incidence of irregular protrusions is also associated with an increased risk of slow flow, potentially due to distal embolisation of lipid core and thrombotic material11. Furthermore, the presence of irregular protrusions is indicative of substantial vessel injury with a high likelihood of medial disruption and lipid core penetration. Previous studies in animals have consistently demonstrated a positive relationship between excessive vascular injury and increased neointimal proliferation12. It is hypothesised that the inflammatory reaction triggered to repair local arterial injury induced by large stent and balloon sizing may lead to accelerated reactive neointimal growth within the stents13.
In conclusion, the OPINION ACS study confirms the value of imaging-guided PCI and the non-inferiority of OFDI versus IVUS. Although the importance of achieving adequate stent expansion in PCI is well established, the study results remind us to stay cautious and avoid overaggressive stent sizing.
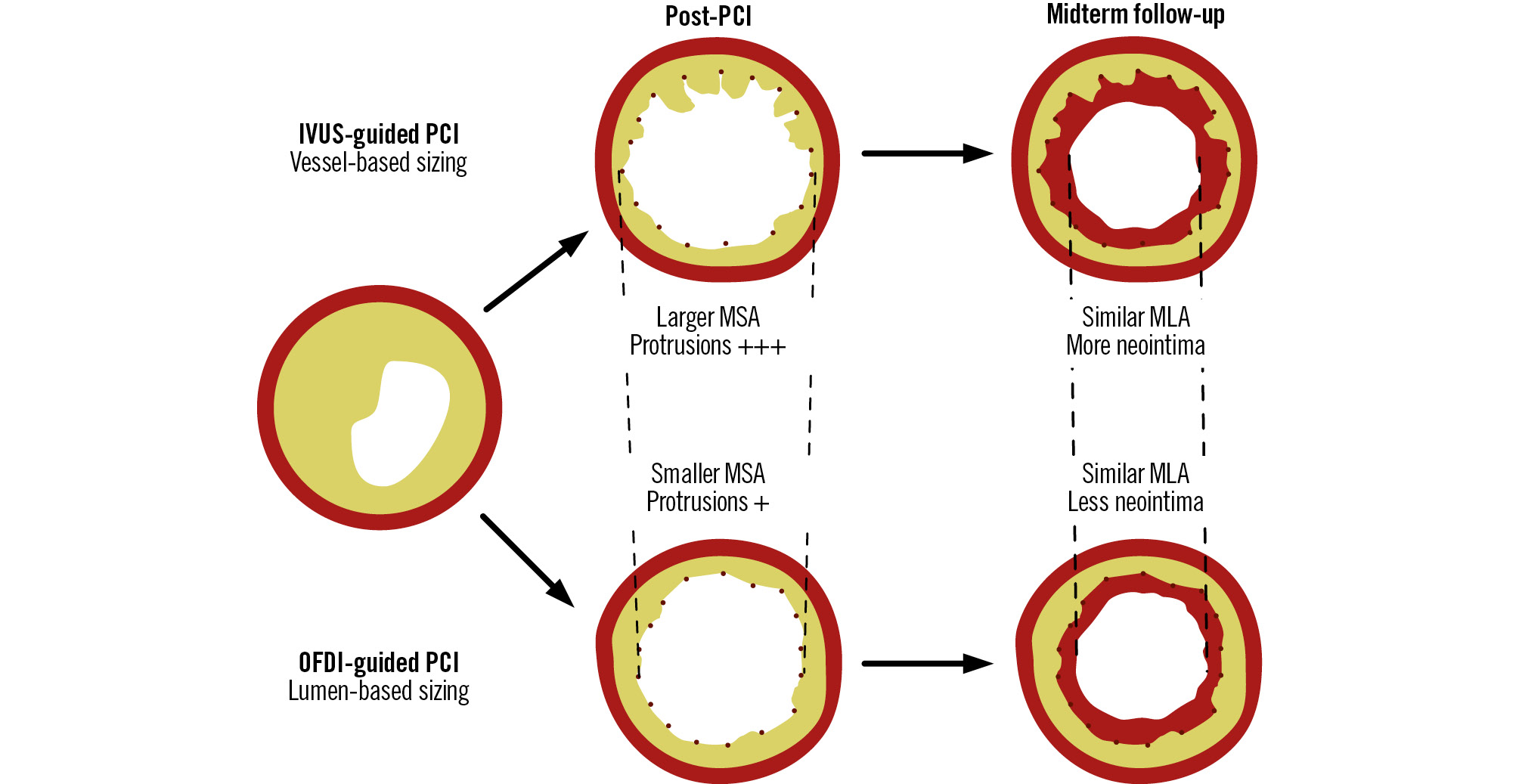
Figure 1. Schematic representation of the effects of lumen- vs vessel-based stent sizing on MSA and MLA, immediately after PCI and at 8-month follow-up. Compared to a vessel-based sizing algorithm (as used in the IVUS arm of the OPINION ACS study; upper row of the figure), a smaller MSA but lower degree of irregular protrusions is observed in the arm where a lumen-based sizing algorithm (using OFDI) was applied. At midterm follow-up (right side of the figure), this eventually leads to a similar MLA due to a less pronounced neointima formation with the less aggressive lumen-based sizing algorithm. IVUS: intravascular ultrasound; MLA: minimum lumen area; MSA: minimum stent area; OFDI: optical frequency domain imaging; PCI: percutaneous coronary intervention
Conflict of interest statement
T. Adriaenssens reports speaker honoraria from Abbott and Gentuity; and is a member of the Gentuity medical advisory board. P. Sinnaeve has no conflicts of interest to declare.