Cory:
Unlock Your AI Assistant Now!
Transcatheter aortic valve implantation (TAVI) is now a widely used treatment for severe aortic stenosis, surpassing isolated surgical aortic valve replacement (SAVR) in many countries. However, hypoattenuated leaflet thickening (HALT) has been observed in 20-30% of TAVI patients, while it is less frequently identified in SAVR patients. Whether this is due to the lack of routine computed tomography (CT) post-SAVR or an actual difference in incidence remains unclear12. The leading hypothesis behind HALT is thrombus formation on valve leaflets, supported by recent histopathological studies that confirm the presence of thrombotic material in HALT lesions3. The primary clinical concerns are whether HALT contributes to thromboembolic events, valve thrombosis, or accelerated structural valve degeneration, and how it should be managed pharmacologically. While empirical anticoagulation has been associated with HALT resolution, its dynamic nature has led many centres to adopt a conservative approach, avoiding the bleeding risks of long-term anticoagulation.
In this issue of EuroIntervention, Grodecki et al present a substudy of the RESOLVE registry, analysing 99 patients who underwent TAVI with balloon-expandable valves (SAPIEN XT or SAPIEN 3 [both Edwards Lifesciences]) and exhibited HALT on a 30-day post-procedure CT scan. They assessed HALT resolution at 1-year follow-up using quantitative thrombus parameters (volume and attenuation in Hounsfield units). Notably, 21% of patients were on anticoagulation at baseline, and only two were switched to anticoagulants after HALT detection4.
A key finding was that higher thrombus attenuation, rather than thrombus volume, was independently associated with HALT resolution. This suggests that thrombus composition plays a crucial role in determining whether HALT persists or resolves over time. Low-attenuation thrombi may represent more acute, less organised clots with red blood cells and fibrin strands, making them more prone to resolution. In contrast, high-attenuation HALT may indicate more organised, chronic thrombi with greater fibrin content, making them more resistant to spontaneous resolution. It would have been interesting to know whether thrombus attenuation also correlated with volume progression or stability versus incomplete resolution, which would further support the study’s findings. However, this information was not provided by the authors. The presence of restricted leaflet motion due to HALT, termed hypoattenuation affecting motion (HAM), was observed in 79% of patients. HAM was associated with both lower thrombus attenuation and larger volume.
Beyond thrombus characteristics, the study also explored the mechanical properties of the prosthesis, assessed by stent frame deformation, and their impact on HALT progression. Parameters such as valve eccentricity, canting, and deformation index were independently associated with HALT resolution, reinforcing the idea that non-linear flow dynamics contribute to thrombus persistence5. Furthermore, low implantation depth and prosthesis eccentricity emerged as predictors of both thrombus burden and HAM, suggesting that suboptimal prosthesis positioning influences both HALT development and progression towards more severe leaflet dysfunction (Figure 1). The association between stent frame deformation and clinical outcomes is becoming increasingly evident. Data from the ACURATE IDE trial suggested a higher stroke risk in patients with underexpansion of the ACURATE neo2 valve (Boston Scientific)6. Similarly, Nagasaka et al reported that underexpansion and eccentricity of the SAPIEN 3/Ultra valves (Edwards Lifesciences) increased the risk of all-cause mortality, stroke, and heart failure readmission, as well as HALT and HAM incidence7. A large cohort study with self-expanding and balloon-expandable TAVI also showed that stent frame deformation was associated with HALT, all-cause mortality, cardiac death, and heart failure readmission8. These findings suggest that suboptimal prosthesis expansion and circularity not only influence HALT development but may also serve as predictors of adverse clinical outcomes.
Finally, the study demonstrated that thrombus volume changes correlated with transvalvular gradient alterations over time. Moreover, structural valve deterioration was associated with larger thrombus volume at 1 year. These results further highlight HALT’s potential clinical relevance to valve durability.
Despite the valuable insights provided by this study, the long-term evolution of HALT remains incompletely understood. Further research is needed to assess the relationship between HALT characteristics and clinical outcomes such as stroke, heart failure, mortality, and valve durability, as well as the response to anticoagulation.
More refined risk stratification based on clinical data and imaging characteristics – such as thrombus attenuation and prosthesis deformation parameters – may help predict HALT evolution and individualise post-TAVI management strategy, balancing the potential benefits of anticoagulation against bleeding risks. Moving forward, a better understanding of HALT’s clinical implications and optimal treatment strategies will be crucial to improving long-term outcomes in TAVI patients.
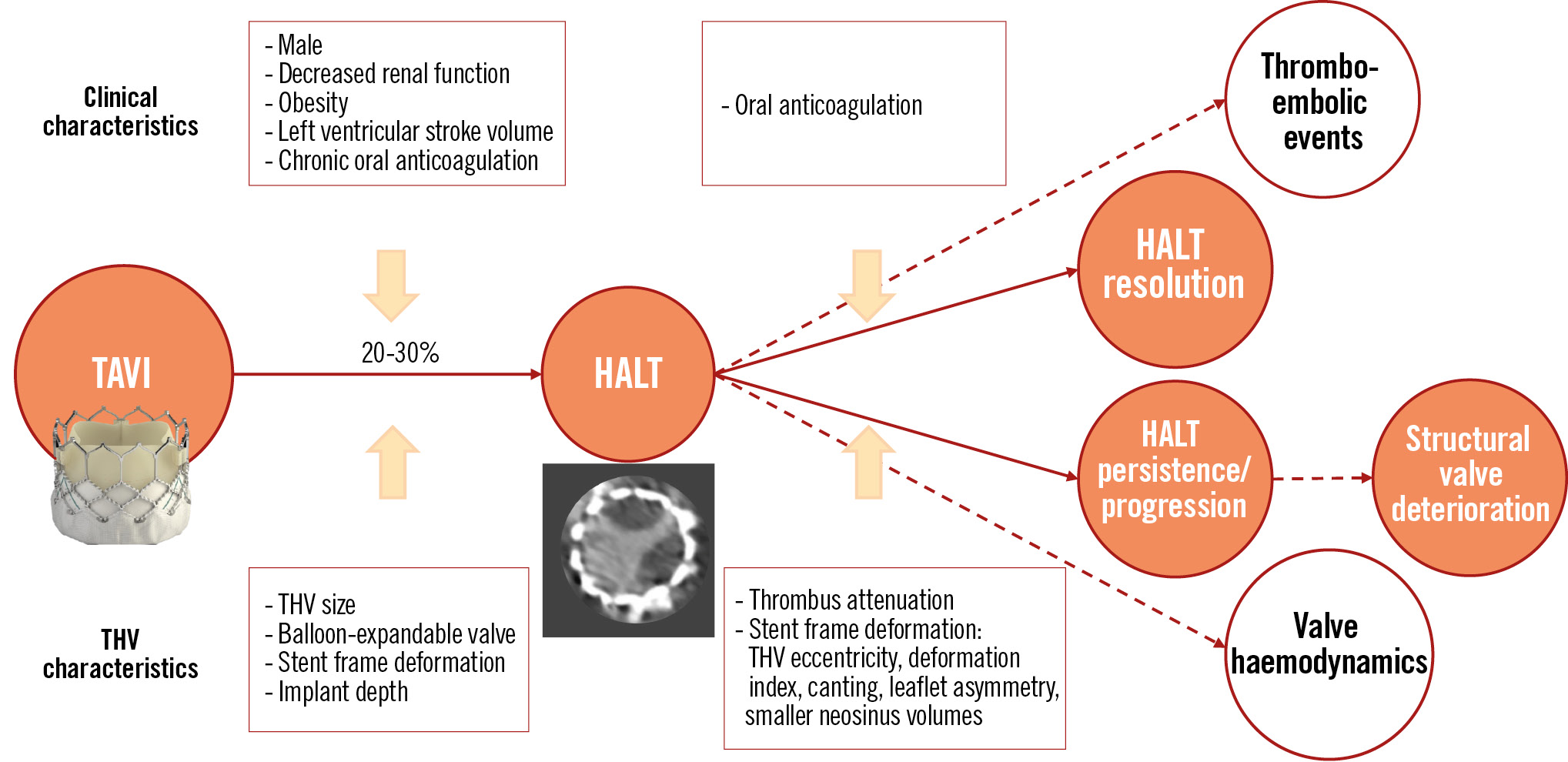
Figure 1. Main factors associated with HALT development and resolution. HALT: hypoattenuated leaflet thickening; TAVI: transcatheter aortic valve implantation; THV: transcatheter heart valve
Conflict of interest statement
The authors have no conflicts of interest to declare.